Hospital: H U 12 de Octubre.
Nº: C2019-679
Aut@r o Autores: S. Nagrani, E. Martínez, P. Encinas, S. Borruel.
Presentación
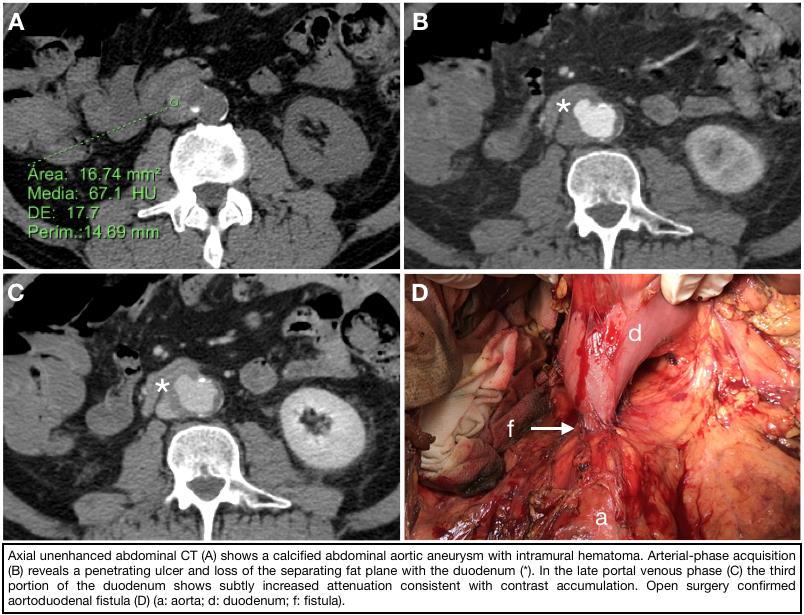
A 65-year-old man with a 2-week history of intermittent vomiting and melena presenting with hematemesis, dizziness, hypotension and weak distal pulses. Acute aortic syndrome was suspected, so triphasic CT aortic angiography was performed (figure), which demonstrated a complicated abdominal aortic aneurysm with enteric fistulazation.
Discusión
Aortoenteric fistula (AEF) is an uncommon but life-threatening condition which consists of an abnormal connection between the aorta and the gastrointestinal (GI) tract, involving the duodenum more frequently. It typically occurs in association with a large atherosclerotic abdominal aneurysm. However, with the development of reconstructive vascular surgical procedures, the incidence of AEF has increased over the last decades as a postoperative complication distinguishing primary AEF (PAEF) from secondary AEF (SAEF). Etiological factors include aneurysm pulsatility against to the bowel wall plus a concomitant low grade inflammatory or infective process with bacteremia involving the aorta/aortic graft. The classical triad of GI bleeding, abdominal pain and pulsating mass is not as frequent as believed. Massive exsanguination is usually preceded by a minor and self-limiting hemorrhage from hours to several months. Hemodynamically unstable patients should be taken directly to the operating room since imaging tests delay proper management. On the contrary, CT angiography should be performed in all hemodynamically stable ones as first-line diagnostic study. Specific CT features include extravasation of aortic contrast into the bowel lumen and leakage of enteric material into the periaortic space. Perigraft or intraluminal gas is highly suggestive of AEF since graft infection is usually caused by intestinal flora from duodenum (anaerobic bacteria is rare). Indirect signs are more common findings and comprise periaortic fluid (< 20 UH) or soft tissue edema (> 20 UH), loss of separating fat plane, disruption of the aortic wall and focal bowel thickening > 5 mm. In cases in which SAEF is suspected, it must be taken into account that any ectopic gas within the aortic wall is abnormal after 3-4 weeks from surgery. Likewise, any perigraft soft-tissue thickening, fluid or hematoma should be resolved within 2-3 months after surgery. Presentation may be unspecific (sepsis, malaise, weight loss, fever of unknown origin…), particularly when there is no frank communication with the GI lumen but graft erosion
Conclusión
AEF is a rare but catastrophic condition that requires prompt diagnosis for patient survival. Contrast extravasation is a specific but low sensitive feature, radiologist should suspect AEF in the presence of periaortic fluid, soft tissue thickening and loss of the separating fat plane with GI tract in symptomatic patients with abdominal aneurysm/prior aortic surgery.
Bibliografía
- Vu QD, Menias CO, Bhalla S, Peterson C, Wang LL, Balfe DM. Aortoenteric fistulas: CT features and potential mimics. Radiographics. 2009,29(1):197-209. - Perks FJ, Gillespie I, Patel D. Multidetector computed tomography imaging of aortoenteric fistula