Hospital: Gerencia de Atención Integrada de Albacete.
Nº: C2019-228
Aut@r o Autores: I. Donoso Esteban, Á. Fernández López, D. Caldevilla Bernardo, A. Ibáñez Ibáñez.
Presentación
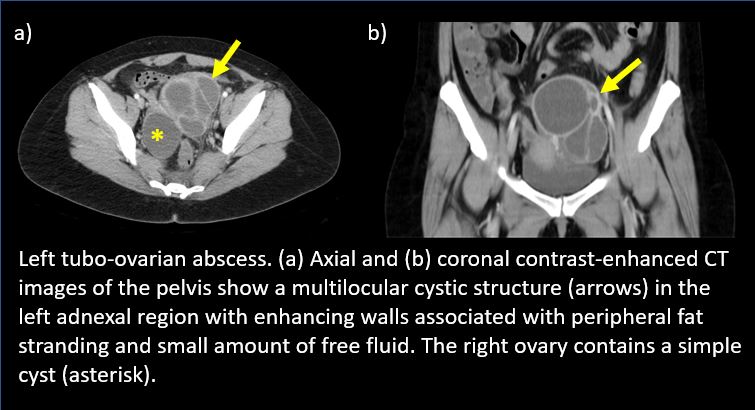
A 35-year-old woman who comes repeatedly to the emergency room due to pain in the hypogastrium and left iliac fossa with 3 days of evolution after performing hysterosalpingography (HSG), with painful cervical mobilization, leukocytosis and fever, negative vaginal cultures and visualizing retrograde annexes with multiloculated lesion with echogenic content compatible with left ovarian abscess by transvaginal ultrasound. To complete the assessment, an urgent abdominal-pelvic CT with intravenous contrast was performed, showing a multilocular cystic structure in the left adnexal region with enhancing walls associated with peripheral fat stranding and lymphadenopathy. The left ovary was not seen. The uterus was normal and a simple cyst in the right ovary was seen. Small amount of free fluid was seen within the pelvis. These findings were compatible with left tubo-ovarian abscess. The patient underwent a laparoscopy, which confirmed a left 15 cm tubo-ovarian abscess, which was adhered to posterior aspect of uterus. A left salpingectomy with oophorectomy was performed.
Discusión
HSG is a fundamental radiological technique in the study of female infertility since it allows the evaluation of the uterus and the fallopian tubes by administering contrast through the cervical ostium. One of the associated complications are infectious conditions such as pelvic inflammatory disease (PID). Tube-ovarian abscesses are one of the complications of PID although they have also been associated with other factors such as intrauterine devices, multiple sexual partners, diabetes mellitus, immunosuppression, uterine surgeries, etc. The clinical context is of great relevance in the radiological interpretation, being an important suspicion diagnosis in patients with pain to vaginal exploration and mobilization of the cervix. CT is essential for the assessment of these complications, with the key tomographic signs being: - Liquid pelvic masses with liquid-liquid or hydro-aerial levels. - Thickened and hyper-captive walls. - Impossibility of distinguishing ovary and tube. As a differential diagnosis we must consider pelvic neoplasms, abscesses in diverticulitis or appendicitis, ovarian torsion, etc.
Conclusión
PID is an important but unusual complication of HSG that should be considered as a diagnostic possibility in patients with pelvic pain and cervical mobilization, and that can present complications such as tube-ovarian abscesses in which the radiologist’s role, and techniques such as CT, are fundamental.
Bibliografía
- Kalish GM, Patel MD, Gunn ML, Dubinsky TJ (2007) Computed tomographic and magnetic resonance features of gynecologic abnormalities in women presenting with acute or chronic abdominal pain. Ultrasound Q 23: 167-175 - - Webb EM, Green GE, Scoutt LM (2004