Hospital: Hospital Universitario de Getafe.
Nº: C2019-699
Aut@r o Autores: E. Escudero Romo, V. San Martín Luque, L. Alonso De Caso García, A. Berral Santana, M.A. Jiménez López, F. Carretero López.
Presentación
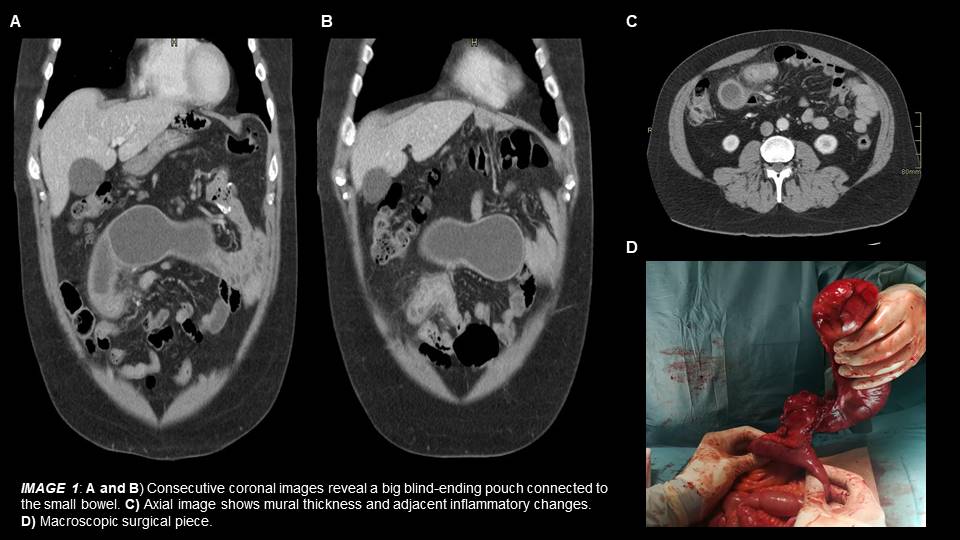
44-year-old male admitted to the emergency department with 10 days of abdominal pain located in the mesogastric area irradiated to the lower abdomen. Physical examination revealed right lower quadrant tenderness and signs of peritoneal irritation. Laboratory tests showed leukocytosis with high number of neutrophils and a C-reactive-protein of 120 mg/dl. An abdominal ultrasound was performed initially showing stranding of the softtissue as unspecific finding, therefore completed with an intravenous contrastenhanced computerized tomography (CT) scan. The CT scan revealed a large size blind-ending saccular structure or pouch connected to a small bowel loop and located in the supraumbilical region. The pouch presented mural thickness, mainly on its source, and associated softtissue inflammatory stranding. The appendix was normal.
Discusión
According to the CT scan findings the first possible diagnosis is a Meckel’s diverticulum showing inflammatory changes, suggesting Meckel’s diverticulitis. Meckel’s diverticulum is the most common congenital gastrointestinal anomaly, due to a persistent remnant of the omphalomesenteric duct. The diverticulum is located on the antimesenteric border of the distal ileum with a length that may reach up to 15 cm. Clinical symptoms arise from complications which accounts for approximately up to 25% Meckel’s cases and are most common in children and male adults. The most frequent complications are gastrointestinal bleeding, obstruction and diverticulitis. Patients with Meckel's diverticulitis and lower abdominal pain often get misdiagnosed with appendicitis. The ultrasound evaluation is of limited value, therefore in the emergency practice CT is the elected technique even though the diverticulum may be indistinguishable from normal small bowel if it’s not complicated, or difficult to discriminate from abscess when it is. On CT scan Meckel’s diverticulitis appears as a blind-ending tubular or round structure of variable size with mural thickening and adjacent soft-tissue inflammatory changes. The fact that the pouch-like structure is attached or continued with the adjacent small bowel loop is clue for the diagnosis. Based on radiological and clinical findings inmediate surgery was required, revealing a giant Meckel’s diverticulum located 50 cm from the ileocecal valvewith inflammatory changes associated. The histologic features confirmed the diagnosis.
Conclusión
Although Meckel’s diverticulum is a rare cause of abdominal pain in adulthood, to be familiar with this possible diagnosis is crucial in cases of abdominal pain on right lower quadrant, specially in appendicectomized patients. Most frequently the radiologic finding of this entity is a blind-ending pouch connected to the ileum, asocciating the radiologic manifestations of its complications.
Bibliografía
1. Chaterjee A, Harmath C, Vendrami CL, Hammond NA, Mittal P, Salen R, et al. Reminiscing on Remnants: Imaging of Meckel Diverticulum and Its Complications in Adults. AJR 2017, 209:287-296.