Hospital: Hospital Universitario 12 de Octubre.
Nº: C2019-188
Aut@r o Autores: L. Ibañez, C. Cruz-Conde, I. Alba, P. Encinas, M. Depetris, E. Martinez.
Presentación
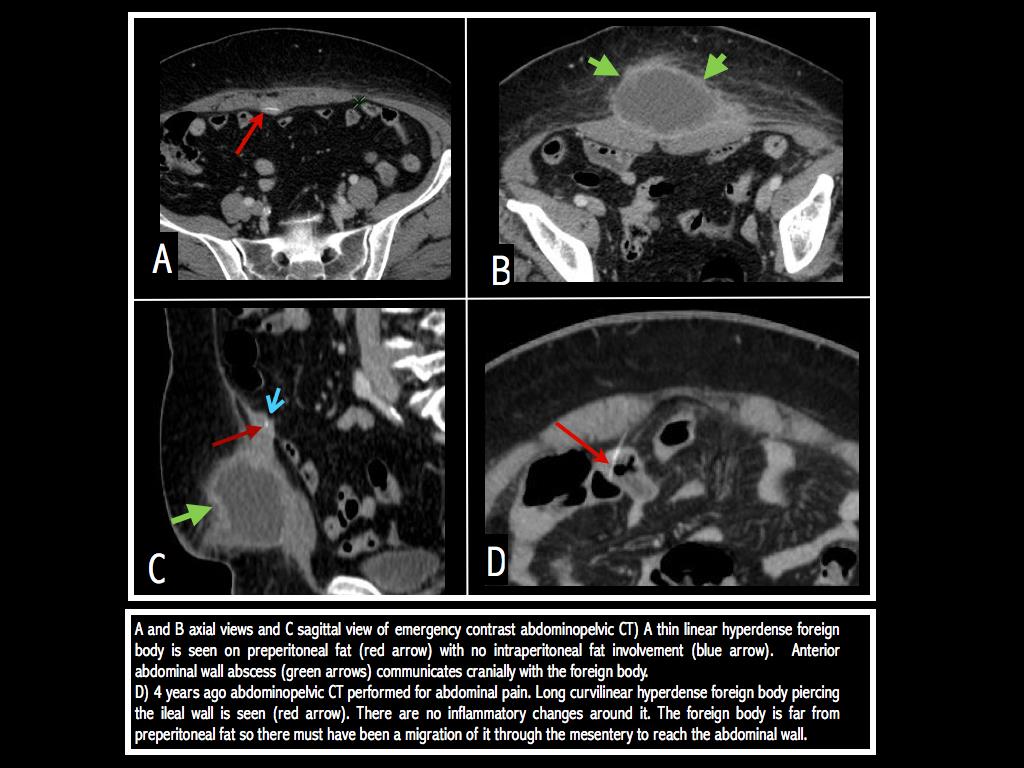
67 yo woman came to the emergency room with a painful, swelling and redness fluctuating mass on the anterior abdominal wall, so an abscess was suspected. An abdominal CT with intravenous contrast was performed. A subcutaneous abdominal wall abscess was shown with a linear hyperdense structure in its deepest part, on preperitoneal fat. The patient denied eating fish recently. A CT performed 4 years ago was reviewed, when the patient consulted for abdominal pain. A linear structure of 4 cm that piercing the through at the small bowel wall at the ileum was observed, compatible with a fishbone and that was not described.
Discusión
Accidental ingestion of a fishbone (FB) is a common clinical issue but the incidence of complications and bowel perforation is extremely low, less than 1%. FB perforation can occur in all segments of the gastrointestinal tract, although it tends to present in regions with acute angulation such as lesser gastric curvature, the second or third portion of the duodenum, or more often at ileocecal (83%) and rectosigmoid junctions. In some patients, the FB may migrate and be seen situated away from the site of perforation. There are some risk factors as cultural habits of consumption of an entire unfilleted fish or the use of dentures that impairs palatal sensory feedback, which identifies sharp and hard-textured items in a food bolus. The clinical presentation could be as acute abdomen with abdominal pain, fever, bowel obstruction, peritoneal irritation, and sepsis, but sometimes the onset of symptoms could be preceded by a long time lag. In these situations, clinical manifestations could be very different like an intra-abdominal or liver abscess and inflammatory lesions mimicking malignancy. The abdominal radiograph is ineffective at diagnosing FB ingestion. Linear hyperreflective foreign bodies could be detected by ultrasound, but it depends on their orientation. CT is useful in detecting complications like fat stranding, abscess, peritoneal effusion, and pneumoperitoneum. A foreign body perforation is usually an unexpected feature, and FB is shown as a thin curvilinear hyperdense lesion so high-quality multiplanar reconstructions and no administration of positive oral contrast are necessary to the diagnosis. If there are intraperitoneal complications, laparoscopy may be performed to remove the FB, drain the abscesses and repair of the perforation.
Conclusión
Thin curvilinear hyperdense lesion associated with inflammatory changes are the key features to suspect a fishbone complication
Bibliografía
- Paixão TSA, Leão RV, de Souza Maciel Rocha Horvat N, Viana PCC, Da Costa Leite C, de Azambuja RL, et al. Abdominal manifestations of fishbone perforation: a pictorial essay. Abdom Radiol. 2017,42(4):1087–95. - Beecher SM, O’Leary DP, McLaughlin R. Diag