Hospital: Hospital Universitario y Politécnico la Fe.
Nº: C2019-726
Aut@r o Autores: M. Garcia-Junco Albacete, R. Teruel Coll, C.F. Muñoz Núñez, P. Calvillo Batllés, A. Oprisan, R.M. Piqueras Olmeda.
Presentación
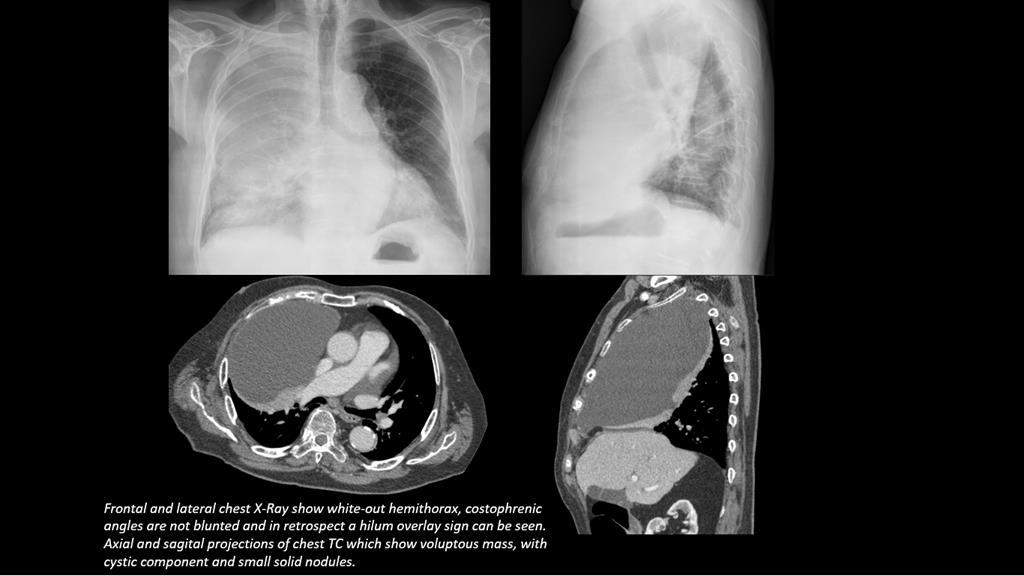
A 91-year-old male presented with a 1-month clinical history of shortness of breath and asthenia. Primary care physician requested a chest X-ray and afterwards the patient was referred to our Hospital Emergency Room (ER). The patient had a previous medical history of dyslipidemia and arterial hypertension and was also a former smoker (50 years ago). He denied fever, cough or expectoration. Blood pressure was of 177/92 mmHg. Pulmonary auscultation showed hypoventilation in the basal right hemithorax. Blood tests were within normal ranges. Chest X-ray showed a right opacified hemithorax and a tumor mass with atelectasis was suspected. A scheduled chest CT was requested. Chest CT showed a voluminous unilocular cystic lesion with small peripheral solid nodules, in anterosuperior location, producing a complete compressive atelectasis of right upper lobe and middle lobe. Extrapleural and mediastinal fat were also affected. The diagnosis offered with CT was a malignant mass originating in the mediastinum (thymic neoplasia) or pleura (mesothelioma).
Discusión
After pathological examination a diagnosis of mesothelioma or atypical mesothelial hyperplasia was established. The high FDG uptake in the PET-CT scan was also a sign of an aggressive lesion. White-out hemithorax is a radiological sign which might appear in the ER and entail a severe pulmonary pathology. Acute or subacute presentations of white-out hemithorax are massive pneumonia (rare), massive obstructive atelectasis, massive pleural effusion or very voluminous masses. In white-out hemithorax mediastinal shift is clue to shorten the differential diagnosis. In obstructive atelectasis the mediastinum will present an ipsilateral shift, except for some atelectasis produced by central pulmonary masses without displacement. Contralateral mediastinal shift may be observed in pulmonary or extrapulmonary masses and is usually described in massive pleural effusion which may require urgent drainage. Finally, pneumonia or pleural malignant mesothelioma typically show no mediastinal displacement. In our case, no mediastinal shift was observed, costophrenic angles were not blunted and in retrospect a hilum overlay sign can be seen pointing to the diagnosis of an anterior mediastinal mass.
Conclusión
Unilateral white-out hemithorax is a radiological sign which differential diagnosis must be mastered by the radiologist, especially to exclude acute and potentially treatable etiologies.
Bibliografía
- S Bharty, B Prakash, M Agarwal, A Bhatnagar. Opaque Hemithorax: Re-Visiting The Causes. The Internet Journal of Pulmonary Medicine. 2013 Volume 14 Number 1. - Gonlugur U, Gin M, Gonlugur T, Mirici A. Unilateral opaque or 'white out' hemithorax. Clin