Hospital: Hospital Serranía de Ronda, Distrito Atención Pirmaria Sevilla.
Nº: C2019-413
Aut@r o Autores: L. Cuesta Lujano, F. Grasa González, I. Pastrano Gallegos, H. Alcarazo Fuensanta, C. Torres Alés, J. Andrades Delgado.
Presentación
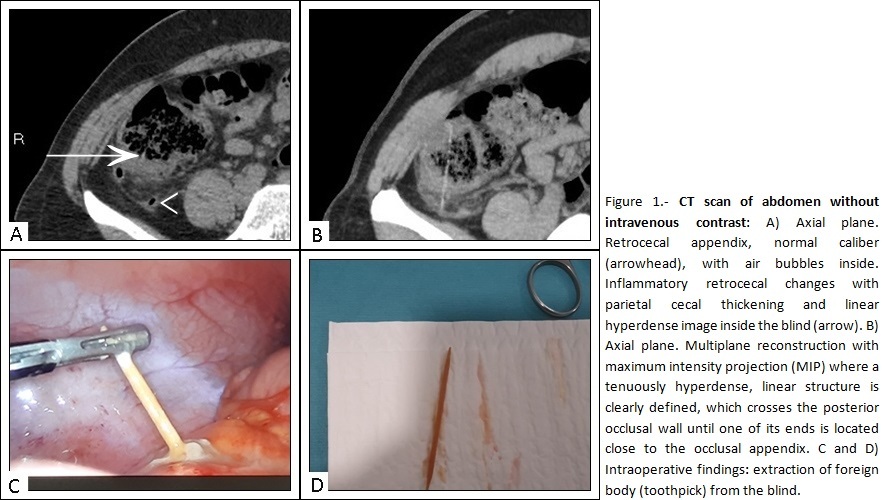
43-year-old woman referred from the Emergency Department for suspected acute appendicitis (pain in right iliac fossa, positive blumberg, fever (37.5º), leukocytosis (16000 U/uL) with neutrophilia and PCR 123). Urgent abdominal ultrasound was performed to identify an inflammatory plastron in the right iliac fossa as well as a short segment of normal caliber cecal appendix. The appendix showed a retrocecal location so we could not fully assess it. In view of the doubt that it was an acute appendicitis, we completed a study with computed tomography (CT) of the abdomen without intravenous contrast (Figure 1). In the CT scan, the appendix had a normal wall thickness and calibre, as well as air bubbles inside, suggesting that it was not obstructed. The findings were not compatible with acute appendicitis but there were retrocecal inflammatory changes, with some extraluminal air microbubbles, which made locoregional microperforation suspicious. Within one of these microbubbles, as well as in some blind segments, a faint linear discontinuous hyperdense image seemed to be appreciated. After multiplying the reconstruction with maximum intensity projection (MIP), a faintly hyperdense, linear structure of 5 cm was clearly defined, which perforated the cecal wall until one of its ends was located close to the cecal appendix. It was a cecal microperforation by foreign body. Emergency surgery was performed by laparoscopy, extracting a toothpick inserted in the blind (Figure 1 C, D)).
Discusión
The toothpick only accounts for 0.1% of hollow viscera perforations by foreign bodies (1) however, by their pointed nature, they are more likely to cause internal organ damage. We must know which are some of the diagnostic keys that will help us to correctly identify them: 1. A correct medical history (last food ingested?) 2. Adequate evaluation of image tests. Locoregional inflammatory changes with or without extraluminal air bubbles should make us suspect it. 3. ATTENTION! We can find different densities, increasing the difficulty when it comes to wood (higher water content) than calcium (bone, fish bone, clam shell...) or metal. 4. Performing multiplanar reconstruction with maximum intensity projection (MIP) is key to diagnosis.
Conclusión
CT has a high sensitivity and specificity for the diagnosis of perforation of hollow viscera by foreign bodies, and even more if we know how to use the tools it provides. Never forget to use multiplanar reconstructions with maximum intensity projection (MIP) in the case of thin materials that are difficult to visualize(toothpick, heavy spine...).
Bibliografía
- Reginelli A, Liguori P, Perrotta V, Annunziata G, Pinto A. Computed Tomographic Detection of Toothpick Perforation of the Jejunum: Case Report and Review of the Literature. Radiol Case Rep. 2016,2(1):17-21. Published 2016 Jan 5. doi:10.2484/rcr.v2i1.52