Hospital: Hospital Universitario de Getafe.
Nº: C2019-753
Aut@r o Autores: N. Guiracoche Papetti, I. Cedrún Sitges, J. Sánchez Reyes, M. Jimenez Lopez.
Presentación
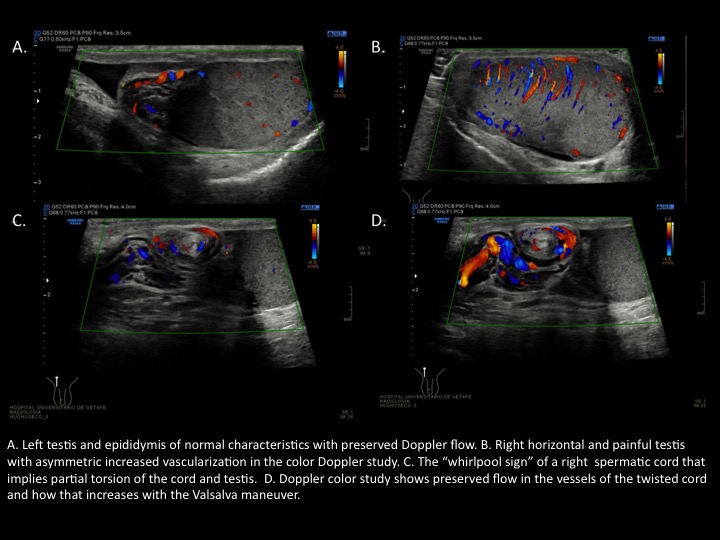
A 21-year-old male attended in the emergency department for acute right testicle pain of 1 hour of evolution. No fever or previous trauma. Physical examination shows right horizontal testicle, painful on palpation. Normal left testicle in scrotal pouch. Testicular Doppler is requested due to clinical suspicion of right testicular torsion In the ultrasound study, horizontal right testicle was observed, of normal size, with homogeneous echogenicity and with vascularization preserved in the color Doppler, discretely increased with respect to the contralateral testicle. Exploring the spermatic cord, a swirling aspect of it is identified. These findings are compatible with cord twisting, probably intravaginal. Left testis and epididymis are of normal characteristics. Discrete bilateral hydrocele. Intraoperative right testicular detorsion and bilateral orchidopexy are performed urgently confirming intravaginal partial torsion.
Discusión
Testicular sonography has contributed greatly to the preoperative diagnosis of testicular torsion and is the mainstay for evaluation of acute scrotal pain. Tipically, an absence of intratesticular flow on color Doppler exam is straightforward diagnostic of testicular torsion however sometimes the flow is preserved, decreased or slightly increased. Testicular torsion is not an all-or-none phenomenon and can be of complete, partial or intermittent types. Complete torsion occurs when the testis twists 360°or greater, usually leading to absence of intratesticular flow on color Doppler exam. Intermittent torsion is defined as sudden onset of unilateral testicular pain of short duration with spontaneous resolution. In partial or incomplete torsion, the degree of spermatic cord twist is less than 360°, allowing for some residual perfusion to the testis (preserved flow). However there is no spontaneous resolution of pain. Within the partial torsions extravaginal torsion type occurs mainly in the firsts years of age and intravaginal torsion type is more common in adolescence. The bell clapper anomaly is the primary risk factor for acute intravaginal torsion. The other ultrasound signs that we have to search for the diagnosis of testicular torsion with preserved flow are the “whirlpool sign”of the spermatic cord, a redundant spermatic cord or horizontal lie of the testis that could be associated with the bell clapper anomaly. Other signs that could be present but that are not specific to testicular torsion and that can be found in other pathologies are globular testicular enlargement, heterogeneous echotexture and epididymal enlargement without hyperemia. Clinical correlation is essential. Severe nausea and vomiting and abrupt pain, suggest torsion. Incomplete testicular torsion is a difficult diagnosis both clinically and sonographically.
Conclusión
The presence of intratesticular flow does not exclude testicular torsion. If the suspicion of testicular torsion is high, we should look for other ultrasound signs that give us the key and thus avoid underdiagnosis of
Bibliografía
- Bandarkar AN, Blask AR. Testicular torsion with preserved flow: key sonographic features and value-added approach to diagnosis. Pediatr Radiol. 2018,48(5):735-744.