Hospital: Hospital La Paz.
Nº: C2019-596
Aut@r o Autores: G. Buitrago Weiland, Á. Díez Tascón, M. Caicoya Boto, F. García Martínez, M. .J. Simón Merlo, M. Martí De Gracia. University
Presentación
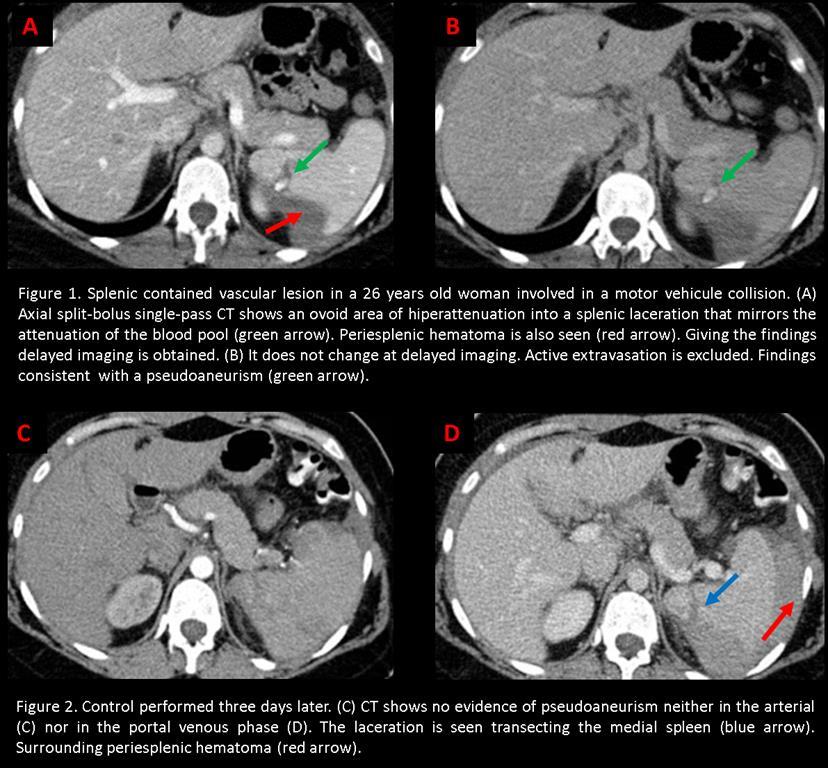
A 26 years old woman is transferred to our emergency room after a traffic-accident (80 km/h). At admission, the patient is hemodynamically stable although she has pain in the left flank. Being a high energy trauma and according to the protocol of our hospital a split-bolus single-pass CT of the abdomen-pelvis is performed. It is observed a splenic laceration with two vascular lesions inside. Aditionally phase is acquired without observing changes in morfology lesions. With the diagnosis of splenic pseudoaneurysms the patient is moved to the vascular room.
Discusión
The presented case corresponds to a high energy trauma with normal vital signs and no apparent injuries. Traumatic injuries are related to the intensity of the transferred energy. They may not be evident at clinical examination, conventional radiology or ultrasound, or may even manifest late. Among these hidden lesions, the most frecuent are delayed hepatic or splenic ruptures secundary to vascular lesions, like pseudoaneurysms. The diagnostic technique of choice for these contained vascular lesions is MDTC. The conventional protocol for its detection must include an arterial phase since a pseudoaneurysm can go unnoticed in the portal phase by de “washing out" phenomenon. The venous phase is necessary to rule out vascular lesiones not contained, such as early and late arterial bleeding, and parenquimal lesions. The combination of the two phases provides a dynamic view of the behavior of the lesions and a better diagnostic performance. The problem is that it imparts to patients, mostly young people, a significant radiation dose with an associated small but significant cancer risk. With the aim of reducing the radiation a single venous phase is usually performed, which, as we have already said, can under-diagnose the pseudoaneuysms. To avoid this problem the split bolus protocol has been devised. It is a contrast medium injection technique that provides both arterial and venous enhancement with a single pass of the CT gantry. The contrast medium injection is divided into two boluses with an initial injection providing solid organ portovenous enhancement and a second bolus giving arterial enhancement. This is the only protocol that in a single helical would allow detecting pseudoaneurysms. The only drawback is that the amount of intravenous contrast used is somewhat higher.
Conclusión
The split-bolus single-pass CT is the diagnostic technique of choice for the search of hidden vascular lesions in young people with blunt abdominal trauma.
Bibliografía
- Jeavons C, Hacking C, Beenen LF, Gunn ML. A review of split-bolus single-pass CT in the assessment of trauma patients. Emerg Radiol 2018, 25: 367-74. - Leung V, Sastry A, Woo TD, Jones HR. Implementation of a split-bolus single-pass CT protocol at a UK