Hospital: Radiology Resident at Hospital Universitario Central de Asturias, Pathology Resident at Hospital Universitario Central de
Nº: C2019-352
Aut@r o Autores: P.A. Rueda Mejía, N. Sordo Alonso, S. Martín García, R. Ugalde Herrá, A. Fernández Del Valle3, M. Tijerín Bueno3.
Presentación
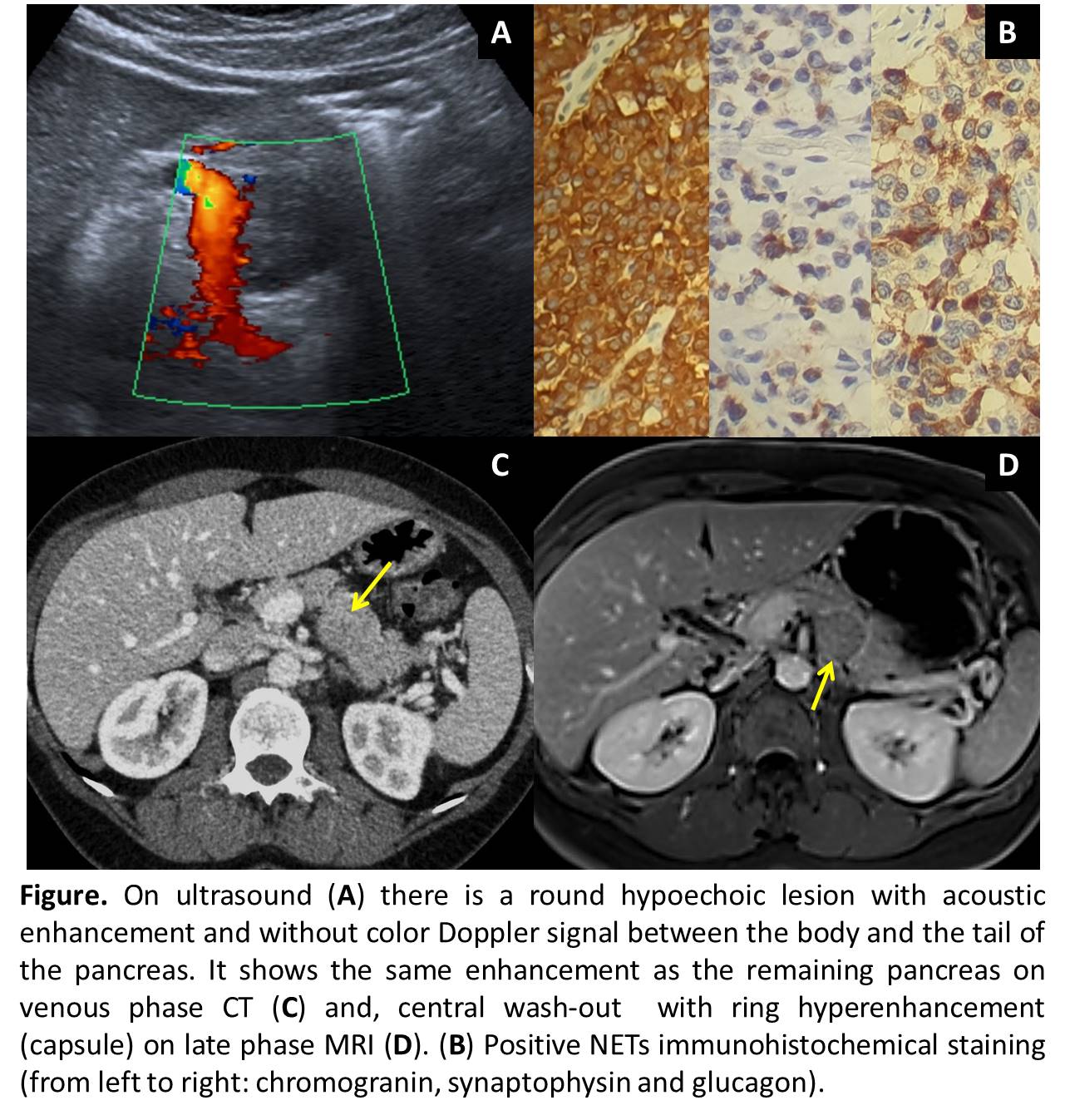
55-year-old woman with family history of stomach and pancreatic cancer came to our hospital due to left nephritic colic symptoms. Abdominal ultrasound showed left hydronephrosis with a stone in the distal ureter. Additionally, we found a round hypoechoic lesion at body-tail pancreas junction, measuring 29x25mm, with acoustic enhancement and without Doppler color signal. The lesion had homogeneous contrast enhancement on CT, similar to the pancreas. MRI showed a solid lesion, with capsule, mild hyperintensity in T2-weighted-images (WI), diffusion restriction, mild contrast enhancement with slow and late wash-out. There is no infiltration of vascular or neighbouring structures and no metastases were found. Those findings reminded of solid pseudopapillary tumor (SPT). However, the pathologist reported a neuroendocrine tumor (NETs), glucagonoma-type.
Discusión
Solid lesions of the pancreas are classified as neoplastic and nonneoplastic. Neoplastic group divides into adenocarcinoma (90%), NETs (1-5%), SPT (1-2%), pancreatoblastoma (0.2%) and pancreatic lymphoma (0.5%)(1). In our case SPT was considered. It’s more common in young women and frequently located in pancreatic tail. Due to the slow growth, it’s usually large at diagnosis with compressive symptoms rather than invasion of adjacent structures. At imaging, it has well-defined edges (pseudocapsule) and progressive enhancement (less than the normal pancreas). It could present hemorrhage (10-18%), cystic degeneration and peripheral calcifications (30%). However, Glucagonoma was pathologically confirmed. It is the third most common functioning NET-type (1%), frequently located in the pancreas body and tail, 70% are malignant with metastases in up to 60% and 52% of 10-years overall survival (10y-OS). NETs share some common distinguishing features. At MRI, most NETs have low signal intensity on T1WI and intermediate to high signal intensity on T2WI. The most distinctive feature is a rich vascular supply with avid contrast enhancement during the arterial phase, more rapidly and intensely than the normal pancreas. Atypical image findings have been reported for glucagonomas, as low signal intensity on T1WI, slightly high signal intensity on T2WI, mild contrast enhance during the arterial phase and wash-out during the venous phase, similar to our case(2).
Conclusión
Most of early stage pancreas tumors are discovered incidentally at imaging performed for an unrelated clinical indication. Accurate and timely imaging diagnosis is essential because it guides clinical management, and improves significantly long-term prognosis (64% of 10y-OS). Therefore, it´s important radiologists do a proper evaluation of any visible structures in all urgent scan techniques, even if it’s not associated to the motive of requesting.
Bibliografía
- Low G, Panu A, Millo N, Leen E. Multimodality Imaging of Neoplastic and Non- neoplastic Solid Lesions of the Pancreas. RadioGraphics. 2011,31:993– 2011. - Lv W, Han J, Liu X, Wang S, Pan B, Xu A. Imaging features of glucagonoma syndrome?: A case report