Hospital: HCUVA.
Nº: C2019-111
Aut@r o Autores: F. Barqueros-Escuer, A. Cuelliga-Gonzalez, Murcia, Spain, J. MartinezMartinez, J. Felices-Farias, Murcia, Spain, G. Litran-Lopez, A. Navarro-Baño,
Presentación
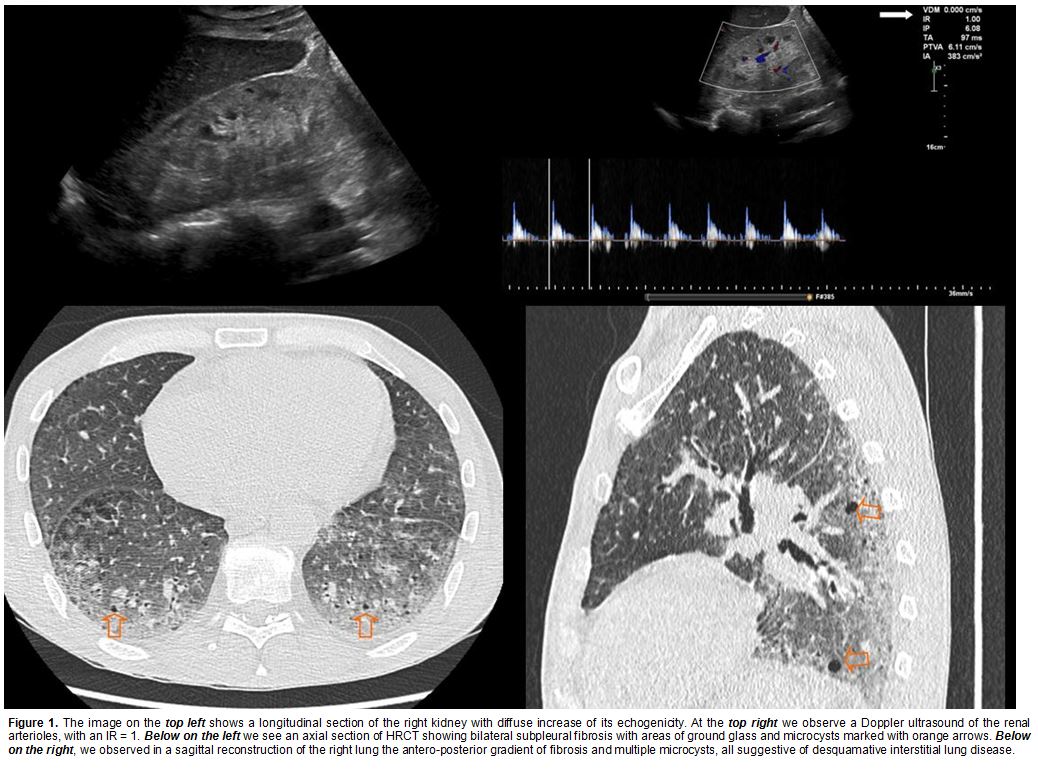
Patient diagnosed in 2015 with diffuse scleroderma (ANA +, anti-SCL70 +) with cutaneous and pulmonary involvement who went to the Emergency department with hypertensive crisis and rapidly progressive renal failure (Cr. 5.5 mg/dL). Abdominal sonography was performed and showed a diffuse increase in bilateral renal cortical echogenicity with loss of cortico-medullary differentiation and a marked increase in the resistance index, which was 1 in both kidneys. With the radiologic findings and lab results, in the context of known diffuse systemic sclerosis, the patient was diagnosed of sclerodermic hypertensive renal failure and acute renal failure, which was treated with hemodialysis, ACEIs and oral corticosteroids.
Discusión
Scleroderma or systemic sclerosis is a rare autoimmune disease that predominantly affects women of middle age (30-50 years of age). This condition causes fibrosis in the skin and subcutaneous tissue and frequently involves the internal organs such as heart, lungs, kidneys, and gastrointestinal tract. Clinical manifestation depends on which systems are predominantly involved. The patient was diagnosed in 2015 with scleroderma anti-SCL70 + and ANA +, with fast progressive skin involvement and with dyspnea of moderate efforts. HRCT was performed and showed diffuse interstitial lung disease with subpleural fibrosis predominance and pulmonary microcysts, all suggestive of desquamative interstitial pneumonia. Currently, the leading causes of death in scleroderma are pulmonary fibrosis and pulmonary arterial hypertension. Scleroderma renal crisis (SRC) has remained one of the most dreaded complications of scleroderma, with incidence ranges between 10% and 20%. However, since the introduction of angiotensin-converting enzyme inhibitors, the mortality and morbidity from SRC have decreased significantly.Renal manifestations of scleroderma are common, affecting up to 25% of patients. The pathophysiology is very similar to malignant nephrosclerosis and is characterized by pronounced constriction of arcuate and interlobular arterioles resulting in focal cortical ischemia.Imaging tests are very useful in the diagnosis of SRC: inflammatory changes, glomerular sclerosis and arteriolitis cause diffuse renal hyperechogenicity on ultrasound. Besides, in contrast enhanced CT, we found spotted nephrogram, an appearance of patchy and subsegmental renal parenchymal enhancement.
Conclusión
- Renal hypertensive crises in patients with scleroderma have decreased in their practice due to ACE inhibitor therapy. - The treatment with ACEI has improved the survival of patients and has reduced the dialysis requirement. - It's important to know
Bibliografía
Steen VD. Scleroderma renal crisis. Rheumatic Disease Clinics of North America, 2003,29(2):315-33. ? Bose N, Chiesa-Vottero A, Chatterjee S. Scleroderma renal crisis. Seminars in Arthritis and Rheumatism, 2015,44(6):687-94.