Hospital: Hospital San Cecilio.
Nº: C2019-303
Aut@r o Autores: M. Valero Gonzalez, I. Garrido Marquez, A. Milena Muñoz, Y. Nuñez Delgado, P. Garcia Villanova Ruiz, M. Eisman Hidalgo.
Presentación
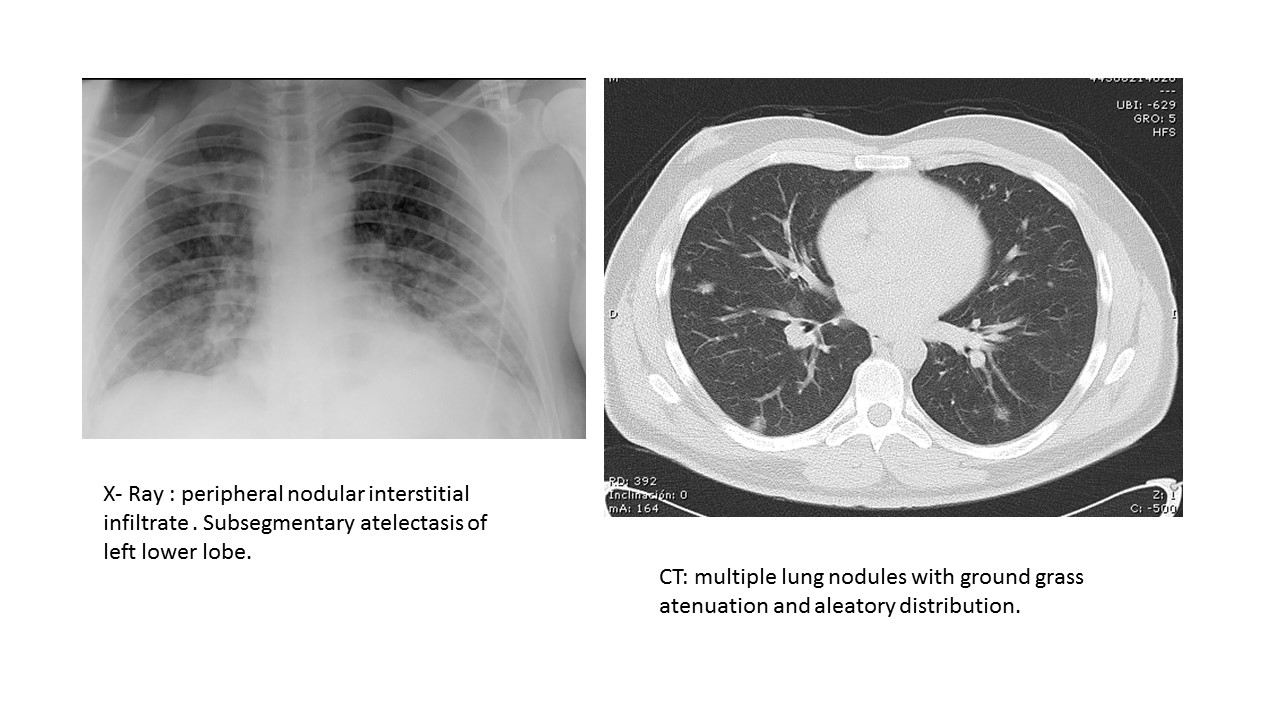
We report a case of atypical measles in an man 36 years old without previous measles immunisation, with rash and serious pulmonary disease that needed mechanical ventilation. The radiological studies were showing multiple ground glass nodules. The evolution was parallel to rash, with simultaneous disappearance of the pulmonary disease and radiological features.
Discusión
Measles is acquired through the respiratory tract with dissemination by lymphatic system. In the first phase the virus replicates at the point of inoculation and reticuloendothelial system. In the second phase it affects the skin, conjunctiva, respiratory tract and other organs. The greatest contagiousness is in prodromes ( 2 to 4 days before the rash to 4 days after) . In Spain, it is considered a notifiable disease and the incidence was 4.49 / million between August 2017 and August 2018, due to antivaccine groups, unvaccinated travelers to endemic areas or unvaccinated children from marginal populations . Clinically it has a prodromes of 2-4 days of cough, coryza, conjunctivitis and high fever. It´s common Koplik spots . After that ,a not pruritic and confluent maculopapular rash develops . In this period the patient suffers most complications. After the fourth day it begins to disappear in the same order in which it appeared. The diagnosis is clinical with serologic confirmation . The main acute complications appear in infants and children up to 9 years and young adults : pneumonias, otitis, laryngopharyngitis, diarrhea, vomiting and encephalitis. Chronically, subacute sclerosing panencephalitis is described years after. Atypical measles syndrome was first described in the 1960s in association with the inactivated measles vaccine, characterised by pneumonia with lobular or segmental infiltrations, hilar lymphadenopathy and pleural effusion. Respiratory measles presents two forms : primary atypical pneumonia due to measles virus and typical neumonía caused by bacterial superinfection. Measles pneumonia appears in 3-4% of patients with more prevalence in pregnant women, haematological malignancies, AIDS or immunosuppressive therapy. Histollogy is a giant cell pneumonia, before or with rash. X-ray shows a peripheral interstitial infiltrate with lobular atelectasis. In CT the most frequent features are patchy consolidation, ground-glass opacification and small centrilobular nodules. It is a risk factor for bronchiectasis. Frequently there are hilar adenopathies and pleural effusion. Although these nodules usually disappear, they can sometimes calcify and persist years after. Bacterial superinfection is more frequent and is caused by S. aureus, pneumococcus, H.influenzae and S. pyogenes, visualizing confluent areas with cavitation and air bronchogram.
Conclusión
Atypical pneumonia is a serious complication of measles and can attends with spherical and segmental consolidations, which can be confused with metastasis or lung sequestration. It is neccesary knowing it for avoiding diagnostic mistakes.
Bibliografía
- Melenotte C, Cassir N, Tessonier L .Atypical measles syndrome in adults: still around. BMJ Case Rep. 2015 Sep 23,2015. pii: bcr2015211054. doi: 10.1136/bcr-2015211054 - Kim EA, Lee KS, Primack SL et al. Viral pneumonias in adults: radiologic and path