Hospital: Hospital General Universitario de Ciudad Real, Hospital Universitario de 12 octubre.
Nº: C2019-742
Aut@r o Autores: M.J. Rodríguez Muñoz, M.A. Depetris, C. Pastor Sánchez, R. Frías García, B. Sánchez Neila, C. Ariza Molina.
Presentación
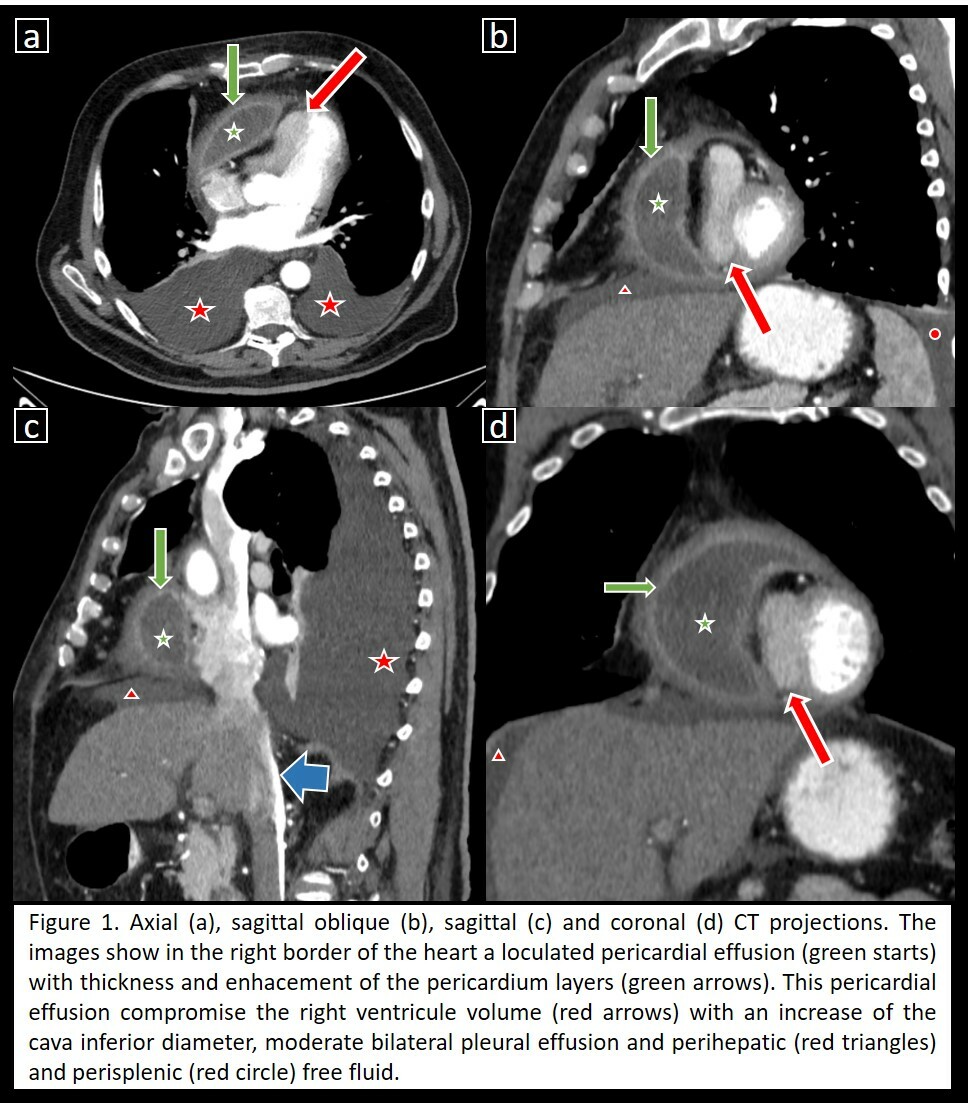
A 59 years old man, with history of myopericarditis the last month, presented asthenia, dyspnea and edema of lower limbs. He has a history of diabetes, dyslipidemia and moderate cognitive impairment (due to this situation he had not administrated himself correctly the medication to myopericarditis). The echocardiogram reveled right ventricular compromise with right ventricle free wall collapse and bulging of the interventricular septum to the left ventricle, the chest X-ray bilateral pleural effusion and low voltage on the electrocardiogram. He didn´t present fever or leukocytosis and was hemodynamically stable. The computed tomography (CT) revealed in the right margin of the heart a loculated pericardial effusion (green starts) with thickness and enhacement of the pericardium layers (green arrows). This pericardial effusion compromised the right ventricule volume (red arrows) with an increase of the cava inferior diameter, moderate bilateral pleural effusion and perihepatic (red triangles) and perisplenic (red circle) free fluid. The patient underwent subtotal pericardiectomy and the pericardial effusion culture detected Staphylococcus aureus. The patient recovered without clinical evidence of heart failure.
Discusión
Purulent pericarditis is infrequent. Infection usually arises from contiguous focus or hematogenous seeding. Primary form is very rare. The common organisms implicated are Staphylococcus, Streptococcus and Mycobacterium. On CT, pericardial layers are thickened with diffuse contrast enhancement and the attenuation of pericardial fluid may be similar to that of water or increased in same cases of exudative or purulent forms. The risk of constrictive pericarditis is relatively frequent in purulent pericarditis, particularly in patients with an incessant course and large pericardial effusions, like our patient. Constrictive pericarditis occurs when the rigid pericardium due to fibrosis and adhesions limits the heart movements. This causes, first, impaired right ventricular filling and can lead to heart failure with peripheral edema, hepatic congestion, as well as ascites. CT imaging shows thickening of the pericardium, pericardial calcifications and signs of heart failure: a dilated right atrium, dilated hepatic veins, dilated inferior vena cava, periportal edema, enlarged superior vena cava to more than the adjacent aorta, reflux of contrast into the inferior vena cava (blue arrow) and distal hepatic veins.
Conclusión
The CT is useful to focus the diagnosis in the pericardium pathology. Purulent pericarditis would be suspected with pericardial effusion and enhancement of the pericardial layers and constrictive pericarditis with thickening and contrast enhancement of the pericardium with signs of heart failure.
Bibliografía
- Wada A, Craft J, Mazzaferri EL. Purulent Pericarditis Leading to Constriction. Cardiol Res.2014,5(6):188-190. - Bogaert J, Francone M. Pericardial disease: value of CT and MR imaging. Radiology 2013,267:340–356. - Restrepo CS, Lemos DF, Velasquez E