Hospital: H U N S C, CHARE-BENALMADENA, PTS SAN CECILIO.
Nº: C2019-546
Aut@r o Autores: P. Garcia-Perez, S. Duque, A. Alvarez-Alriols3, A. Carrion, J. Gonzalez-Ortega4, B. Baudet. HUVN,
Presentación
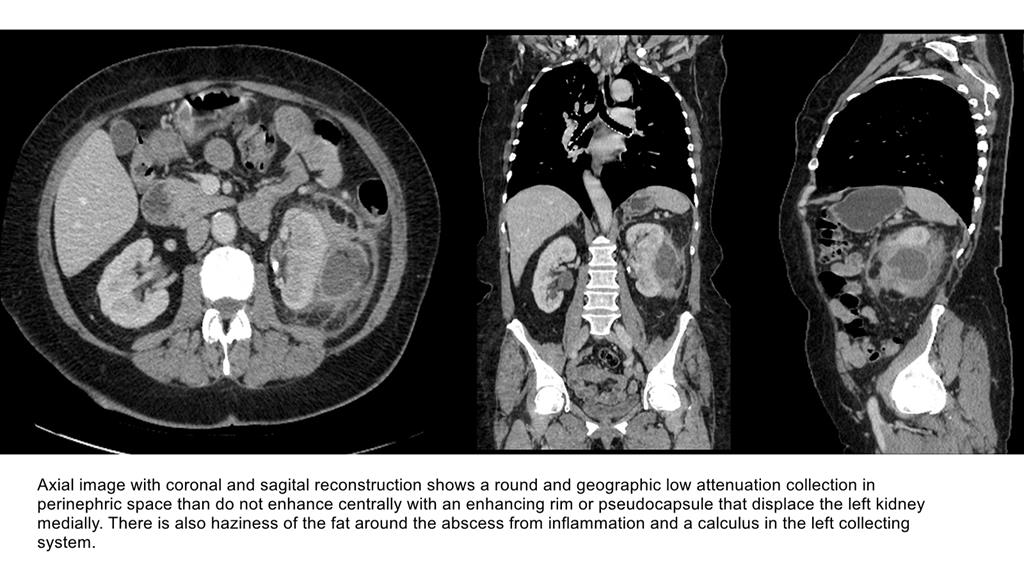
We present the case of a 60-year-old diabetic woman with history of diverticulitis, renal litiasis and urinary infections who was attended in the emergency room for left abdominal pain, and episodes of vomiting, and diarrhea in the last 1 month. Laboratory tests showed anemia, slight leukocytosis, elevated erythrocyte sedimentation rate, and elevated C-reactive protein levels. With the suspected diagnosis of diverticulitis, CT was requested. CT images showed enlargement of the kidney, mild dilatation of the pelvicaliceal system with a renal and ureteral calculus, perinephric fat stranding, thickening of Gerota fascia, and a round low-attenuation perinephric collection with an enhancing rim, being diagnosed of perinephric abscess.
Discusión
Perinephric abscess is an uncommon complication of urinary tract infections. The incidence ranges from 1-10/10000 hospital admissions. Perinephric abscesses usually occur because of disruption of a corticomedullary intranephric renal abscess, recurrent pyelonephritis, xanthogranulomatous pyelonephritis or an obstructing renal pelvic stone causing pyonephrosis. Gram negative bacterial abscess commonly develops due to rupture of corticomedullary abscess while the staphylococcal infection develops due to rupture of a renal cortical abscess (1,2). Factors associated with antimicrobial treatment failure are large abscesses, obstructive uropathy, severe vesico-ureteral reflux, diabetes, old age and urosepsis with gas forming organisms (2). Patients with diabetes mellitus account for about 33% of all perinephric abscess cases and occurs more often insidiously as a secondary phenomenon to upper tract urosepsis, classically in association with an infective renal calculus. The atypical clinical behavior of the diabetic patient has been associated with neurogenic bladder dysfunction of diabetics, greater presence of anatomical alterations of the urinary tract (cystocele, rectocele) and impaired leukocyte function (2). Depending on chronicity, aetiology and complications, perinephric abscess may mimic a tumour radiologically if chronic, or may present dramatically as an acute emergency and mandate evacuation usually with imaged guided pertutaneus drainage.Making a diagnosis promptly and accurately is very important because a delay can result in increased morbidity and even mortality (3).
Conclusión
Abscess within the perinephric space can present a diagnostic challenge. This entity should be considered in the differential diagnosis of any patient presenting with fever and abdominal pain or flank pain or in cases of urinary tract infection that fails to respond promptly to antibiotic therapy, particularly in those known to have renal litiasis and diabetes mellitus. CT is the best modality for fully evaluating the secondary signs of renal inflammatory disease and its complications.
Bibliografía
- William D. Craig, CDR, MC, USN, Brent J. Wagner, MD Mark D. Travis, LCDR, MC, USN . Pyelonephritis: Radiologic Pathologic review. Radiographic 2008, 25:255276. - Robert A. Gardiner, Raymond A. Gwynne and Sally A. Roberts. Perinephric abscess.BJU In