Hospital: Hospital Clínic.
Nº: C2019-518
Aut@r o Autores: G. Isus Olivé, D. Corominas, C. Zwanzger, A. Páez, M. Pages.
Presentación
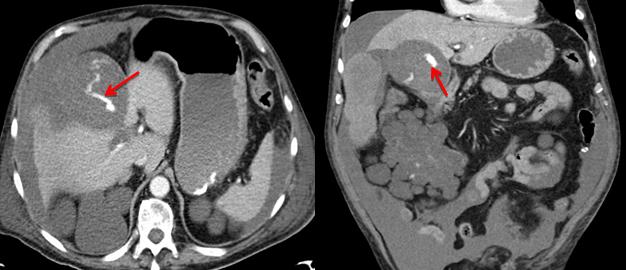
76-year-old man with the following medical history: - Ischemic heart disease - Coronary by-pass surgery - Arterial hypertension - Chronic renal insufficiency due to due to polycystic kidney. Kidney transplant of a donor corpse was performed on 20/7/2018 with no postsurgical complications. During his hospitalization, on August 6, the patient presented sudden diffuse abdominal pain, more intense on the right flank. According to physical examination, the patient was shocked, sweaty and hypotensive, with signs of peritoneal irritation. An ECG was performed, with normal results. Due to the clinical findings, a CT-scan was requested. CT-scan shows a distended gallbladder that contains hyperdense material compatible with blood and clots. A wall defect is also seen, consistent with perforation that conditions hemocoleperitoneum. A contrast extravasation focus inside the gallblader was observed in arterial phase and increased in late phases, compatible with active bleeding. All these findings were suggestive of a hemorrhagic perforated cholecystitis with hemoperitoneum. The anatomopathological analysis was consistent with severe chronic cholecystitis. The patient evolved favorably and asymptomatic, thus, antibiotics and abdominal postsurgery drainages were removed.
Discusión
Hemorrhagic cholecystitis is a rare and serious complication of acute cholecystitis (812%), being vesicular perforation with associated hemoperitoneum even more infrequent (2-11%). The mortality of perforated hemorrhagic cholecystitis raises up to 70%. It is more frequent to occur in a lithiasic vesicle, although it can also happen if it is not.It’s most frequent etiology is due to mural vessels atherosclerosis.Most frequent predisposing factors are anticoagulation, hemorrhagic diathesis, malignancy or trauma. In this context, an episode of acute cholecystitis ends up in vesicular bleeding, parietal necrosis, mural ulceration and rupture. The clinical presentation of hemorrhagic cholecystitis is very similar to acute cholecystitis. In some cases, Quinke triad (abdominal pain in the right flank, painful jaundice and hematemesis) may suggest cystic artery pseudoaneurysm. Ultrasound and CT are indicated for the diagnosis and characterization of this pathology. Cholecystectomy is the definitive treatment of this entity. Cholecystostomy is also performed in some patients who are too unstable to stand surgery. However, even patients with advanced age with multiple medical comorbidities can be successfully treated by surgery.
Conclusión
Hemorrhagic cholecystitis is a rare entity with a high mortality rate, so its early diagnosis by multiphasic CT is of great importance for its subsequent management and treatment.
Bibliografía
- Bolívar-rodríguez, et al. Colecistitis hemorrágica: reporte de caso y revisión de la literatura.(2019).(Vol. 71). - K. Tavernaraki, et al. Massive intraperitoneal bleeding due to hemorrhagic cholecystitis and gallbladder rup