Hospital: Hospital General Universitario Jose Maria Morales Meseguer, Hospital General Santa Lucia.
Nº: C2019-336
Aut@r o Autores: A. García Chiclano, A. Blanco Barrio, I. González Moreno, C. Botia Gónzalez, M.J. Gayán Belmonte, I. Vicente Zapata.
Presentación
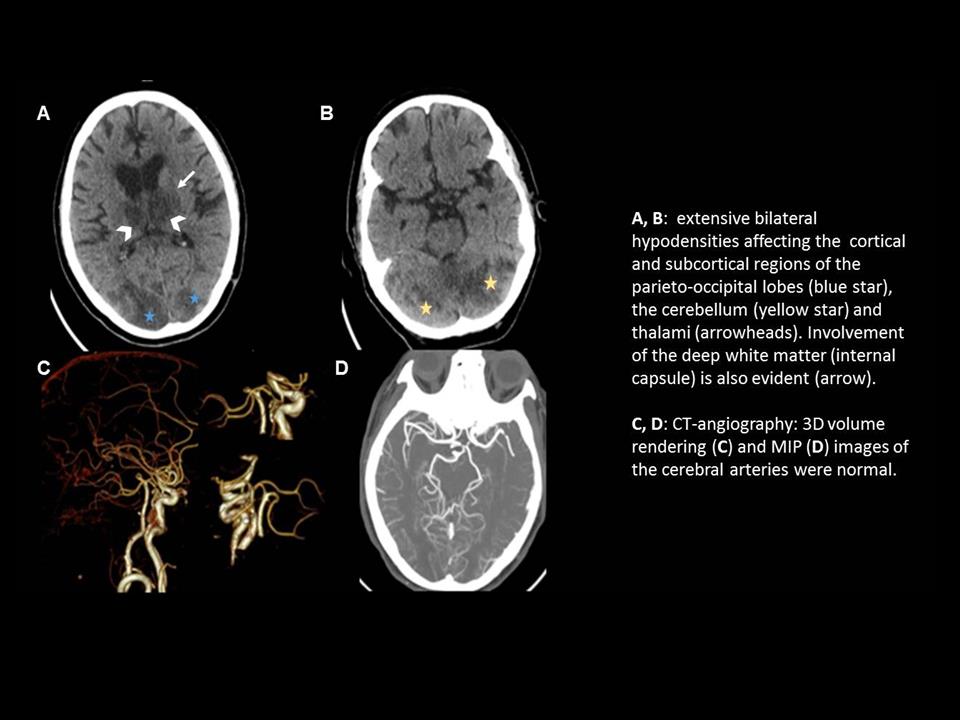
76-year-old woman with no medical history of interest presents with neurological deterioration, hypertension and headache after hip fracture surgery. Brain CT revealed bilateral and symmetrical cortical and subcortical hypodensities in the parietal and occipital lobes, superior cerebellum and both thalami, with associated involvement of the deep white matter. Initial suspicion was a stroke of the posterior territory (top of the basilar syndrome), but CT-angiography did not confirm any filling defect. After blood pressure control, the patient started to improve and became asymptomatic.
Discusión
Diagnosis: Posterior reversible encephalopathy syndrome (PRES). PRES is a radioclinical entity associated with nonspecific neurological symptoms (headache, seizures, impairment of alertness, visual disturbances...).It occurs in evocative clinical conditions (hypertension, eclampsia, immunosuppressor agents, systemic lupus erythematosus...). The typical imaging finding is vasogenic edema predominantly affecting the subcortical white matter of the parieto-occipital lobes (= 98%), often extending to the cortical surface, sparing the deep white matter (unlike our case). There is usually additional involvement of the frontal lobes (˜ 70%), temporal region (˜ 65%) and cerebellum (30-53%). Less common involved areas include the thalamus (˜ 30%), basal ganglia (11,8-34%) and brainstem (12,5-27%). Lesions are mainly symmetrical (71%), but can be asymmetric and even completely unilateral, simulating neoplasm. The posterior areas of the cerebral hemispheres are particularly susceptible. Possible cause would be reduced sympathetic innervation in the posterior circulation, compared to the anterior (more densely innervated by the superior cervical ganglion), rendering the posterior regions less protected from excessive vasodilation and hyperperfusion. ( 1 )Differential diagnosis: - Vascular - Cerebral venous sinus thrombosis - Intracranial hemorrhage - Posterior circulation stroke - Primary central nervous system vasculitis - Non-vascular - Infective encephalitis - Autoimmune encephalitis - Metabolic/toxic encephalopathy Improved knowledge of factors influencing PRES will result in better early management. Delayed diagnosis and treatment may lead to mortality or irreversible neurological deficit. In hypertension associated with drug-induced PRES, treatment includes withdrawal of the drug, immediate blood pressure control, anticonvulsant therapy and, if necessary, temporary renal replacement therapy (hemodialysis / peritoneal dialysis). PRES symptoms usually resolve within a week of presentation if the triggering condition is treated. Radiologic resolution can take weeks despite more rapid clinical recovery. Persistent neurologic deficits have been reported, but are rare.
Conclusión
PRES may be suspected on the basis of history but the clinical findings are nonspecific making diagnosis difficult to establish. Recognition of the characteristic imaging findings by radiologists is the key to diagnose this syndrome.
Bibliografía
- Fugate JE, et al. Posterior reversible encephalopathy syndrome: clinical and radiological manifestations, pathophysiology, and outstanding questions. Lancet Neurol. 2015,14(9):914–25. - Fischer M, et al. Posterior reversible encephalopathy syndrome. J