
Hospital: Hospital Clínico Universitario de Valladolid
Nº: C2019-409
Aut@r o Autores: C. Castañeda Cruz, S. Joral Del Hoyo, T. Álvarez De Eulate García, R. Sigüenza González, J. Rodríguez Jimenez, J.C. M. I..
Presentación
68 years old women arrives to Emergency service, with sudden dyspnea and oppressive centrothoracic pain, of sudden onset while she was resting. When she reached emergency department, that pain had migrated to the interscapular region, with partial improvement after analgesic medication. Troponins were in the high limit of normality. D Dimer was anormaly raised. An angiotc of pulmonary arteries was requested with the clinical suspicion of pulmonary thromboembolism (TEP). In the basal phase without intravenous contrast (iv), a hyperdense area was observed, which included ascending aorta, aortic arch and descending aorta, this area was not enhanced by the subsequent administration of intravenous contrast. This finding suggested the possibility of intramural hematoma. An image suggestive of atherosclerotic ulcer/small aneurysm at the level of the aortic arch was also identified (figure 1). 9 days later, surgical intervention was performed in order to treat the penetrating aortic ulcer, distal to the left subclavian artery exit. However, she returned to the emergency room 20 days after her first visit to this service, with symptoms similar to the first episode, of 7 hours of evolution this time. In this new study, a Stanford type A aortic dissection was identified, which began proximal to the aortic arch and extended to the right coronary artery and appeared to affect the brachiocephalic arterial trunk
Discusión
Due to their possible fatal consequences, such as rupture, acute non-traumatic emergencies that affect the thoracic aorta have been included within the same entity, called “acute aortic syndrome”. The Acute aortic disease is a critical clinical situation whose prognosis usually depends on an accurate and quick diagnosis, as well as the early establishment of its treatment. This communication will focus on the aortic intramural hematoma, its physiopathological mechanisms, clinical characteristics, possible complications such as aortic dissection and the assessment of radiological findings in the emergency department.
Conclusión
The radiologist must know and provide an accurate, quick and detailed diagnosis of acute aortic syndrom, which will allow to guide the treatment (conservative or interventionist) in this entities, with have a high mortality, requiring urgent management.
Bibliografía
- Chao C, Walker G, Kalva S. Natural History and CT Appearances of Aortic Intramural Hematoma. RadioGraphics 2009, 29:791–804 - McMahon M, Squirrell C. Multidetector CT of Aortic Dissection: A Pictorial Review. RadioGraphics 2010, 30:445–460
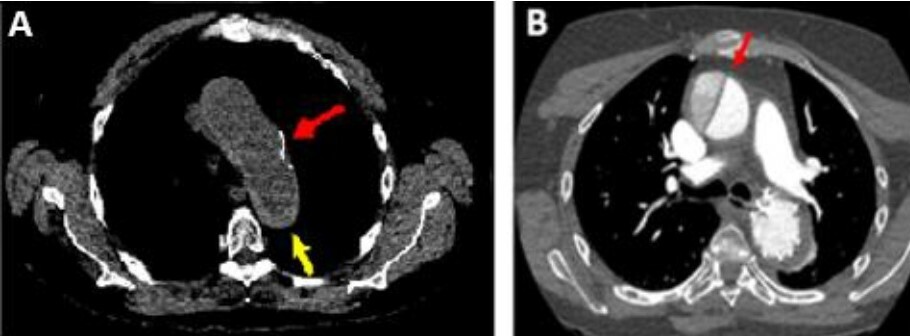
Figure 1: A, Yellow arrow: intramural hematoma, red arrow: penetrating aortic ulceration. B, Red arrow: Stanford A dissection