Hospital: Hospital Universitari Mútua Terrassa.
Nº: C2019-695
Aut@r o Autores: I. Juanico, J. Moreno, A. Pedrerol, N. Egea, J. González, J. Farelo.
Presentación
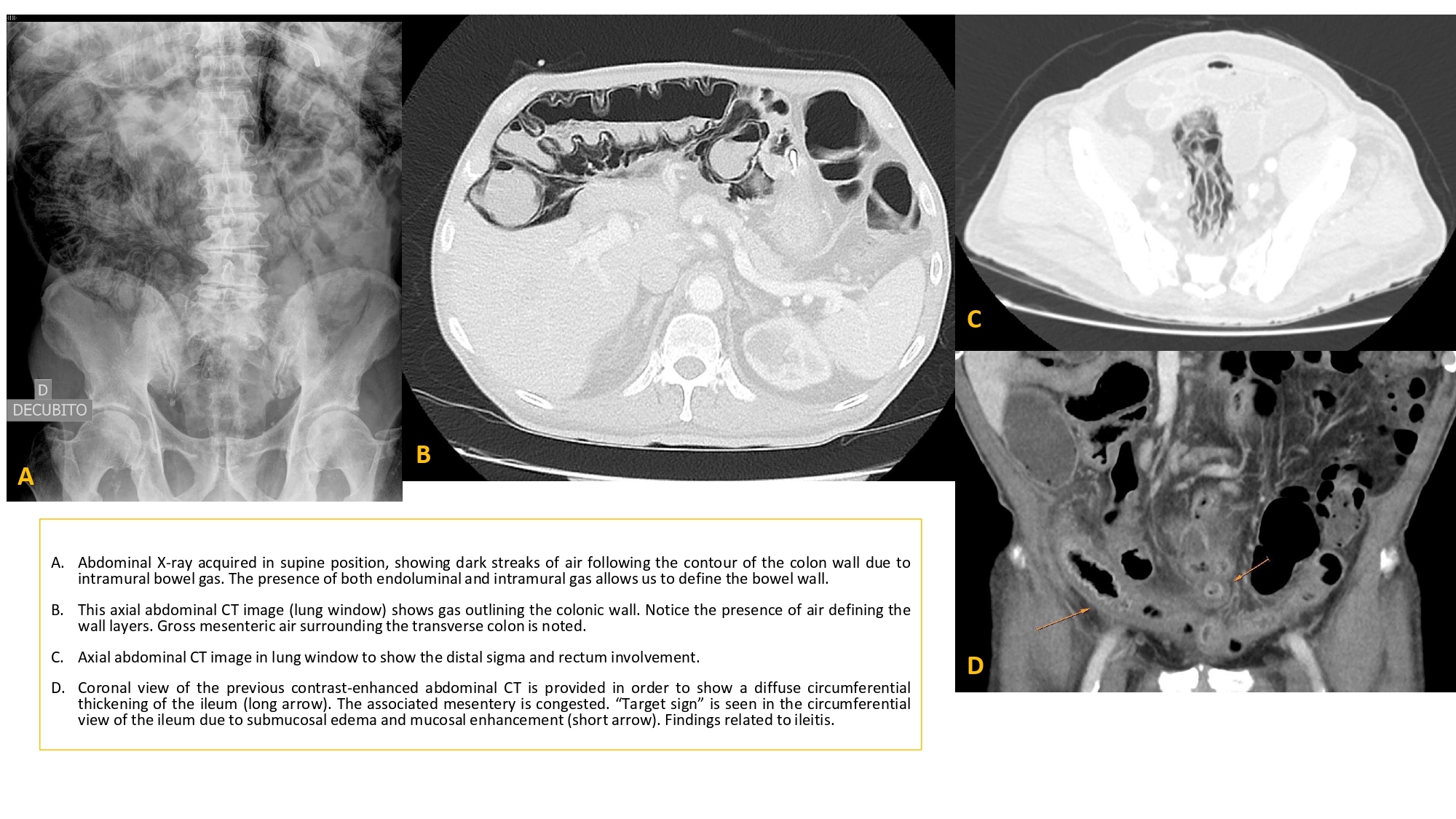
A 75 yo male diagnosed with Crohn’s disease presents an ileitis episode during hospitalization. Corticosteroidtreatment with Methylprednisolone was administered. A CT colonography was performed a few days after and it showed massive presence of air within the terminal ileum wall, the colon and the rectum-sigma.
Discusión
Intramural bowel gas can be identified in the small bowel and the colon, referring to pneumatosis intestinalis (PI) and pneumatosis coli (PC), respectively. This is a result from an underlying pathologic process, ranging from benign to severe and surgical conditions. Intramural gas can be seen in intestinal ischemia, traumatic mechanisms, inflammatory, autoimmune and infectious conditions and pulmonary issues. It can also be induced by drugs, such as corticosteroids, among others. Corticosteroids lead to a certain grade of immunosuppression. When the mucosal or immune barriers in the gastrointestinal (GI) tract are compromised, bacterial intrusion or gas diffusion into the wall becomes more likely. This case illustrates an example of PC and PI due to a compromise of mucosal and immune barriers as a result of inflammatory bowel disease and immunosuression. Intramural bowel gas is a radiological finding characterized by radiolucency within the GI tract wall on plain radiography and by bright echoes on ultrasound. However, computed tomography (CT) is the best imaging modality for establishing this condition due to its greater sensitivity. CT scan distinguishes intramural and intraluminal gas. Furthermore it provides an excellent survey of associated pathologic conditions. Some imaging findings are helpful to distinguish severe causes from benign ones, such as dilated bowel, bowel wall thickening or abnormal wall enhancement. Furthermore, findings like pneumoperitoneum / pneumoretroperitoneum or portal venous gas have been associated with perforation and ischemic bowel. Moreover, the extension of PI does not correlate with the severity of the underlying disease and symptoms. One final practical point is that there are certain findings that can mimicpneumatosis such as gas trapped between the bowel wall and luminal contents, gas trapped by opposing mucosal folds and gas bubbles adherent to bowel wall.
Conclusión
There are many underlying conditions that can lead to PI or PC, ranging from benign diseases to severe conditions that may require surgery. In the same way, clinical context is important to address this patients, as in this particular case. Finally, despite there are some clear radiological findings to detect it, there are some pitfalls to be aware of.
Bibliografía
- Peter SD, Abbas MA, Kelly KA. The spectrum of pneumatosis intestinalis. Arch Surg 2003,138: 68–75.