Hospital: Ramón y Cajal Hospital
Nº: C2019-631
Aut@r o Autores: J. Montilla López-Gay, C. Campos, I. Pecharromán, B. Lumbreras, P. Marazuela García, N. Almeida Arostegui.
Presentación
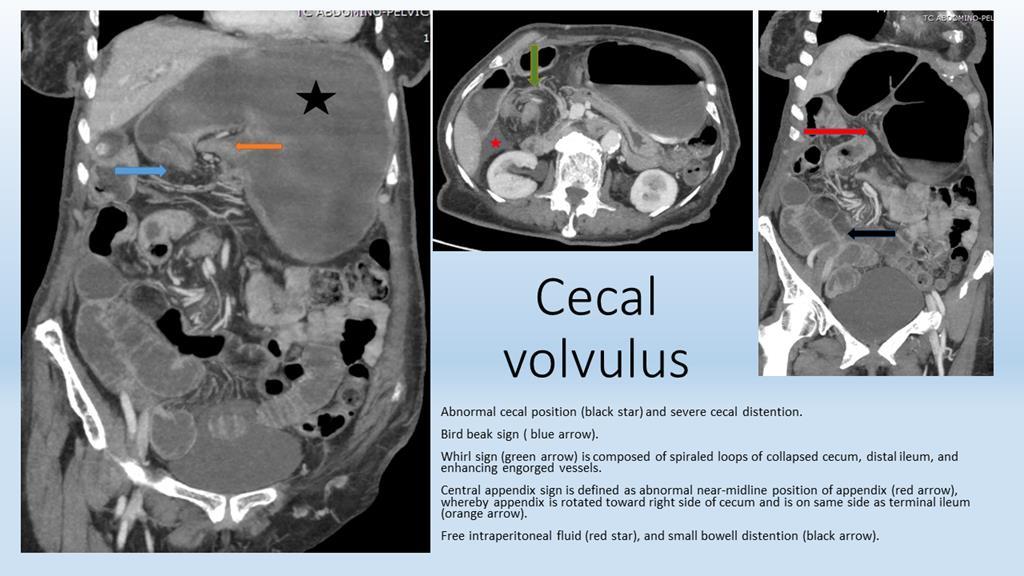
An 86-years-old patient went to the emergency department for vomiting and absence of deposition. On abdominal radiography, signs of intestinal obstruction are visualized. It reveals a loop of distended bowel with haustral creases in the upper left quadrant. On CT it is verified that this image corresponds with a cecal distention, located in an abnormal position. The whirl sign is identified, a specific CT sign for volvulus defined as collapsed loops of cecum with swirling strands of soft tissue, vessels, and fat attenuation centrally. The two limbs of the looped obstruction gradually taper and converge at the site of the torsion, resulting in the appearance of a bird's beak. The terminal ileum is also twisted along with the cecum, conditioning a small bowel obstruction. We can see also the central appendix sign, defined as an abnormal position of the appendix. The small bowel wall appears thickened and surrounded by increased density mesenteric fat, and there is free intraperitoneal fluid.
Discusión
Cecal volvulus consists of a bowel twist involving the cecum, the ascending colon and sometimes the terminal ileum, often resulting in a closed-loop obstruction. In approximately half of the patients the cecum twists in the axial plane, and appearing in the right lower quadrant. The other half of patients have what is known as the loop type of cecal volvulus, in which the cecum both twists and inverts, occupying the left upper quadrant of the abdomen (our case). The plain radiographic features of a cecal volvulus are characteristic. CT evidence the abnormal dilated cecum and confirm its ectopic location. Important signs to look for are the “whirl sign” and the “beak sign”. Multiplanar and three-dimensional reconstructions should complete exam review. Image analysis should also focus on the potential evolution towards severe complications: ischemia of the bowel wall (with thickening and absent contrast enhancement), free intraperitoneal fluid as an initial sign of mechanical ileum failure, and free intraperitoneal gas due to pneumatosisintestinalis in cases of late diagnosis.
Conclusión
Cecal volvulus is the second most frequent localization of colonic volvulus and represents 1-3% of the causes of obstruction of the large intestine in adults. Patients present with nausea, vomiting, constipation and acute cramping pain. The clinical differential diagnosis is usually bowel obstruction versus appendicitis, inflammatory bowel disease or irritable bowel syndrome. CT reveals the presence and location of the volvulus and gives the added benefit of allowing early identification of potentially fatal complications.Surgery represents the treatment of choice for cecal volvulus.
Bibliografía
- Moore CJ, Corl FM, Fishman EK. CT of cecal volvulus: unravelling the image. American Journal of Radiology 2001, 177:95-98. - Tonerini M, Pancrazi F, Lorenzi S, Pacciardi F, Ruschi F, et al.Cecal volvulus: what the radiologist needs to know. Glob Surg 20