Hospital: Hospital Universitario Virgen Macarena.
Nº: C2019-688
Aut@r o Autores: R. Estelles López, X. Cortés Sañudo, C. Pérez Ramírez, P. Rodríguez García, M. Mayorga Pineda, L. Zurita Segura.
Presentación
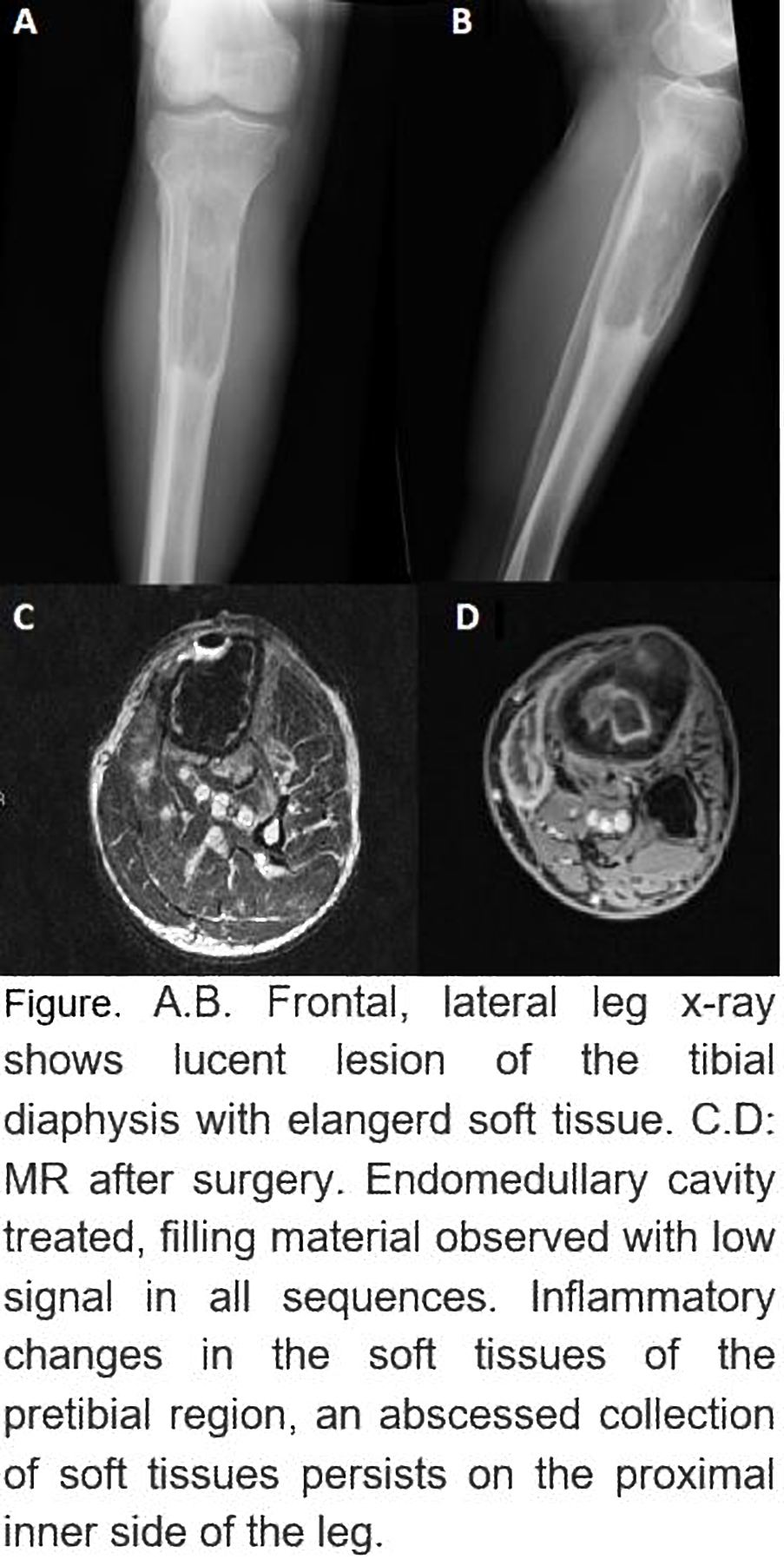
A 77-year-old man consulted at emergency services due to right leg pain without traumatic history. On physical examination, right pretibial swelling, fluctuating, of approximately 5x4 cm, with inflammatory signs. Discrete elevation of CRP. Simple right leg X-ray shows enlarged soft tissue at the anterior face with an eccentric lithic image on tibial diaphysis that causes slight periosteal reaction, with peripheral sclerosis and a narrow, well-defined transition zone. Surgical drainage of fluctuant area was made, with evacuation of purulent material. Mycobacterium CRP positive and microscopic study compatible with mycobacteria. In post-surgical MR, intramedullary cavity treated with low-signal filling material was observed in sequences which maintained a linear peripheral contrast enhancement. Inflammatory changes are also visible in soft tissues of pretibial region, in relation to post-surgical area, an abscessed collection of soft tissues on inner side of proximal leg and knee, following the semitendinosus tendon pathway towards posterior aspect of the knee.
Discusión
Tuberculous osteomyelitis (TBO) is infrequent, when it does occur, femur, tibia, and small bones of hands and feet are most commonly affected. Despite the difficulty of making a precise diagnosis by image only, given the non-specificity of it, the simple Xray continues being the initial diagnostic imaging test. The initial radiologic appearance of TBO is similar to another types of osteomyelitis and includes osteolysis foci with varying degrees of eburnation and periostitis. TBO of long diaphyseal bones will show an increased radio-opacity due to sclerotic bone tissue, more evident when it encompasses a sequestration zone. For definitive diagnosis it is essential to perform a biopsy. MRI imaging findings of acute osteomyelitis are due to edema and formation of exudate in the medullary cavity and are characterized by poorly defined low signal in T1 enhanced sequences and high signal on T2, DP and STIR enhanced sequences, not being possible to delimit the interface between healthy and affected bone marrow. These sequences present a greater sensitivity to detect acute osteomyelitis signs, although they do not allow a precise distinction between edema and necrosis, and it is possible to overdiagnose osteomyelitis, since those signs can also be seen in other entities which develop bone marrow edema such as reactive medullary edema, avascular necrosis, primary or metastatic tumors, fractures and contusions.
Conclusión
TBO is an infrequent entity although it must be considered when dealing with a reemerging disease in our environment. The clinical correlation is essential in its diagnosis since the radiological findings can be indistinguishable from those of other pathologies
Bibliografía
- Burrill J, Williams C, Bain G, Conder G, Hine A, Misra R. Tuberculosis: A Radiologic Review. RadioGraphics. 2007,27(5):1255-1273. - Harisinghani M, McLoud T, Shepard J, Ko J, Shroff M, Mueller P. Tuberculosis from Head to Toe. RadioGraphics. 2000,20(2)