Hospital: Hospital 12 de Octubre.
Nº: C2019-206
Aut@r o Autores: J. Alonso Sanchez, C. Cruz-Conde, J. Garcia Prieto, G. Garcia Galarraga, V. Geronimo Aguilar, E. Martinez Chamorro.
Presentación
A 81 year-old woman was admitted at the Emergency department with bilious vomiting and left flank pain. She denied fever and changes in bowel transit. Laboratory findings showed elevated liver enzymes, leukocytosis and worsening of the renal function. The patient had had previous events of uncomplicated gallstone attack treated with no invasive procedures.
Discusión
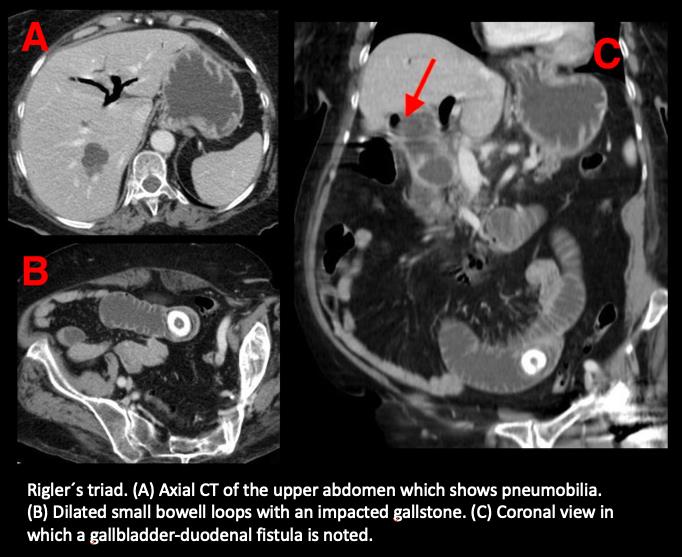
A CT was initially performed with the suspicion of intestinal obstruction. Images provided showed pneumobilia (Image A) and dilated bowel loops with a calcified lesion at the ileum which seemed the most likely cause of the obstruction (Image B). A gallbladder-duodenal fistula was noted in coronal view (Image C, red arrow). These three findings combined re known as Rigler´s triad.Biliary ileus is an uncommon entity which consists in a mechanical obstruction secondary to a gallstone impaction within the gastrointestinal tract. This entity accounts for approximately 1% of all small bowel obstruction and the majority of gallstone ileus patients correspond to elderly female patients. There is a special entity called Bouveret´s syndrome in which the gallstone is impacted within the duodenum. Clinical manifestations, although they may be non specific, are usually preceded by biliary symptoms such as gallstone attack or acute cholecystitis. These inflammatory changes lead to the formation of adhesions and erosion through the gallbladder wall creating fistula to the gastrointestinal tract. A gallbladder-duodenal fistula is the most common finding (due to its proximity) although stomach, small bowel and transverse colon can be affected.When a gallstone migrates along the gastrointestinal tract, it may produced an interrumption of the gastrointestinal tract and cause symptoms of an obstruction such as nausea, vomiting, abdominal pain and abdominal distention . The main therapeutic approach is surgical although there is no consensus in which surgical procedure is best: 1) Enterolithotomy, 2) Enterolithotomy, cholecystectomy and fistula repair in one procedure 3) Enterolithotomy with cholecystectomy and fistular repair in two stages.
Conclusión
Biliary ileus is an uncommon entity in which diagnosis is usually made by CT, which is considered superior than plain abdominal radiograph and abdominal ultrasound. Radiological findings include what is known as Rigler´s triad which consists in pneumobilia, dilatated bowel loops and a gallstone outside its normal location. CT is also useful to describe the location and characteristics of the fistula as in this case.
Bibliografía
- Nuño-Guzman C. Gallstone ileus, clinical presentation, diagnostic and treatment approach. World J Gastrointest Surg 2016, 8(1):65. - Ravikumar R, Williams J. The operative management of gallstone ileus. Ann R Coll Surg Engl 2010, 92(4):279-281.