Hospital: Hospital Universitario Virgen de las Nieves.
Nº: C2019-95
Aut@r o Autores: M. Pérez García, A. García Salguero, M. Rabadán Caravaca, A. Medina Benítez.
Presentación
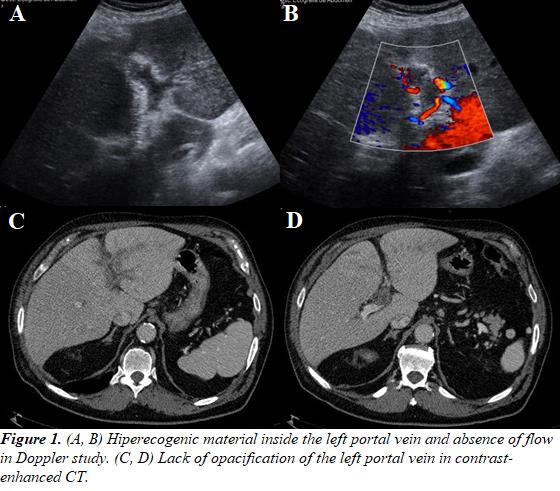
A 78-year-old male with a medical history of POCD presented to the Emergency Department with fever of 6 days with no other symptoms associated. The patient referred a sting by a greater weever (Trachinus draco) 3 weeks before on his left hand, which appeared discretely edematous. Laboratory tests showed acute-phase reactants elevated with no correlating focus in the physical examination or complementary studies performed. The patient was discharged after the prescription of antibiotics. After four days, the patient returned with persistent fever and acute abdominal pain localized in the right upper quadrant. An abdominal US was performed, demonstrating left hepatic lobe hypertrophy with hiperecogenic material inside the left portal vein and absence of flow in color-Doppler study. No collateral vascularization was observed. No other findings were described except perihepatic laminar fluid. A contrast-enhanced CT scan confirmed the portal thrombosis without evidence of thoracic or abdominal tumor. Blood cultures grew Bacteroides fragilis, being pylephlebitis the final diagnosis, for which the patient was prescribed metronidazole and acenocoumarol.
Discusión
Acute portal vein thrombosis is an uncommon finding as an emergency, being usually associated with cirrhosis or tumor. Pylephlebitis or septic thrombosis is a rare cause, as a result of an abdominal infection and bacteremia, being Bacteroides fragilis one of the microorganisms more frequently involved. It usually presents with fever and abdominal pain, as well as leukocytosis. Diverticulitis is the main cause, although appendicitis and pancreatitis are also commonly associated. In some cases, as occurs in this patient, a source of abdominal infection cannot be determined. Ultrasound can be useful as a first diagnostic approach, showing heterogeneous material inside the vessel and absence of flow. Contrast-enhanced CT scan confirms the unopacified portal vein and is also helpful in the assessment of the primary source of infection and possible complications. Being acute, no collateral vascularization will be visualized.
Conclusión
When studying a patient with portal vein thrombosis in the context of fever and abdominal pain, pylephlebitis should be considered as a differential diagnosis. Imaging techniques such as ultrasound and CT scan will confirm the thrombus and can also identify its cause.
Bibliografía
- Balthazar EJ, Gollapudi P. Septic thrombophlebitis of the mesenteric and portal veins: CT imaging. J Comput Assist Tomogr 2000, 24:755–760. - Jha RC, Khera SS. Portal Vein Thrombosis: Imaging the Spectrum of Disease With an Emphasis on MRI Features. AJ