Hospital: Hospital Universitario La Paz, Hopsital Universitario La Paz.
Nº: C2019-556
Aut@r o Autores: S. Agudo Fernández1, Á. Díez Tascón, G. Buitrago Weiland1, M. Martí De Gracia
Presentación
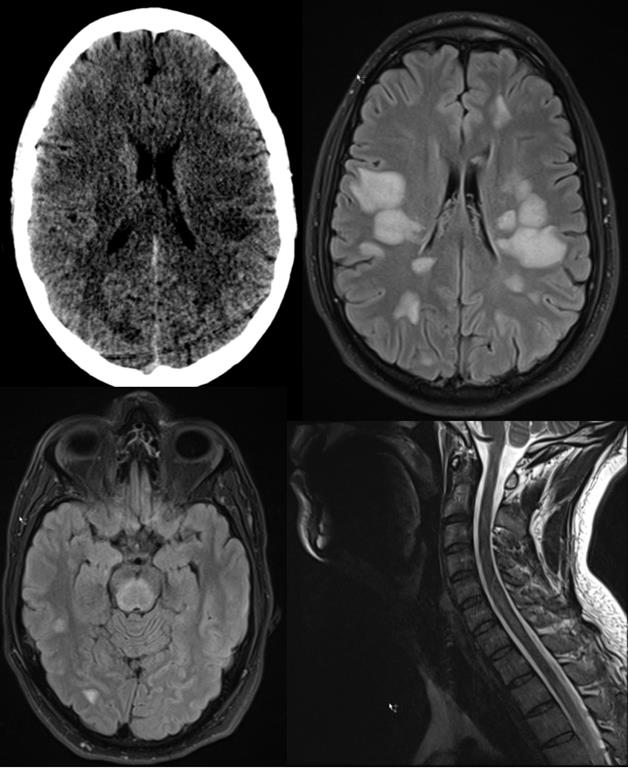
33 year old male arrives to the emergency room because of blurred vision. There is not any relevant allergic or personal history. In the neurological examination he shows peripheral facial paralysis, upper left limb motor weakness, and dysarthria .This was preceded by an upper respiratory tract illness which started 5 days before. Brain stem stroke syndrome is suspected. A brain CT in which ambiguous supratentorial subcortical hypodensities without any vascular pattern are observed is performed. It is supplemented with a brain Angio CT, which does not show occlusion in intracraneal vessels. The rest of complementary tests show normal results. Clinic symptoms having persisted for 8 hours, the brain CT is repeated and it confirms the previously deduced results. A brain MRI is performed. Hyperintense lessions in pons, cerebellar peduncles and supratentorial cerebral white matter are seen on T2weighted and fluid attenuated inversion recovery (FLAIR) sequences. These findings suggest ADEM as the first diagnostic option.
Discusión
ADEM is an acute inflammatory demyelinating disorder mediated by antigenantibodies. It manifests within a two-weeks period after an antigenic challenge, infection, or vaccination. Common clinical manifestations include encephalopathy, fever, headache, seizure, multiple focal deficits, and meningeal signs. (1)(2) The initial exploration which can show focal or multifocal white matter damage or nothing is head CT. (3) RM is the image modality diagnosis chosen, although the initial emergency CT exploration is necessary in order to discard other conditions. On MRI, ADEM lesions are hyperintense on T2-weighted and FLAIR sequences and are usually inconspicuous on unenhanced T1-weighted sequences. With diffusion-weighted MRI imaging (DWI), lesions associated with ADEM show restricted diffusion in the acute stage. (1) Lesions in ADEM are multiple and bilateral and can involve both brain and spine, and both white matter and gray matter. Compared to multiple sclerosis lesions, ADEM lesions can be more rounded and large, with poorly defined margins and more prominent involvement of the deep gray matter nuclei, thalamus, and brainstem. As a reflection of the monophasic course of ADEM, MR imaging should not reveal signs of previous white matter demyelination. (1)
Conclusión
ADEM is a disease included within the spectrum of demyelinating white matter diseases. It requires an Emergency CT in order to discard other neurological syndromes. To later establish the diagnosis, an RM is necessary.
Bibliografía
- Sarbu, N., Shih, R. Y., Jones, R. V., Horkayne-Szakaly, I., Oleaga, L., & Smirniotopoulos, J. G. White matter diseases with radiologic-pathologic correlation. Radiographics (2016), 36(5), 1426-1447. - Garcia, P. M. Sustancia blanca en RM. Congreso Na