MOTIVO DE CONSULTA-SOSPECHA DIAGNÓSTICA
SINCOPE
CARACTERÍSTICAS CLINICAS
Pérdida brusca y transitoria de consciencia con recuperación espontánea en unos minutos, acompañado de signos de alarma, principalmente cefalea y focalidad neurológica. Sin antecedente de TCE previo.
FACTORES MODULADORES / FACTORES DE RIESGO
En relación a los Antecedentes personales:
- Edad avanzada (>65)
- Cardiopatía. Hipertensión arterial.
- Tto anticoagulante, alteración de la coagulación.
- Aneurisma cerebral conocido/intervenido, ateroesclerosis carotidea, MAV.
- Hábito tabáquico. Consumo de cocaína o medicación vasoactiva.
- Embarazo-puerperio, anticonceptivos orales.
- No historia previa de síncopes.
En relación a las Características del Síncope:
- Inicio brusco, sin pródromos.
- Durante / tras esfuerzo. Especialmente al levantar pesos.
- Duración prolongada, difícil recuperación.
- Precedido / acompañado de cefalea intensa (la mayor de su vida)
- Acompañado de náuseas y vómitos brucos.
FACTORES DE ALARMA
Pérdida de consciencia precedido / acompañado de:
- Cefalea intensa /súbita/ persistente.
- Focalidad neurológica (sin criterio de código ICTUS).
- Vértigo, ataxia, diplopía, alteraciones visuales.
- Somnolencia / bajo nivel de consciencia.
- Alteración del comportamiento, estado confusional.
- Emergencia HTA (alteración orgánica grave con riesgo vital).
- Hemorragia retiniana.
- Signos meníngeos.
OTRAS EXPLORACIONES
-Constantes Vitales : TA, FC, FR, Sat. O2, Temperatura, Glucemia.
-Exploración Física y Neurológica rigurosa.
-ECG: arritmias, bloqueos, datos de isquemia aguda, pericarditis, sobrecarga derecha.
–Análisis de Sangre: BQ, HRF, Coagulación (INR) Valorar: MDM, Dímero D, Tóxicos.
-Rx Tórax PA- LAT: datos de taponamiento cardiaco, derrame pleural, cardiomegalia, fallo cardiaco, infiltrado infeccioso.
-TAC cerebral sin/con contraste. Su principal utilidad es para descartar la existencia de sangrado intra o extracraneal, con o sin MAV asociada, así como otras lesiones cerebrales.
-Estudios dirigidos: Holter, Electrofisiología, Ecocardiograma, Prueba de esfuerzo, Mesa basculante, EEG, RM cerebral, TAC torácico, etc.
REGLAS DE PREDICCION CLINICA
No se obtuvieron RPC.
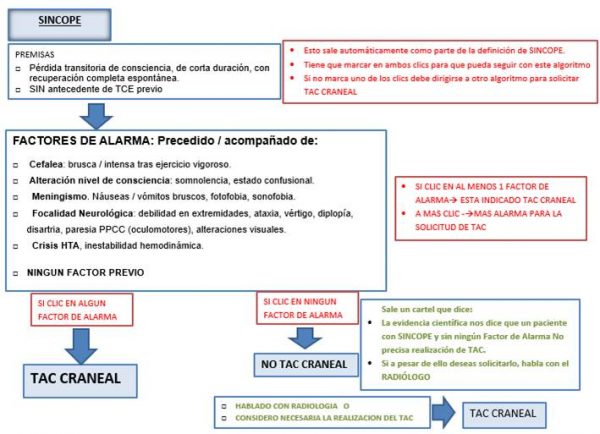
ALGORITMO PROPUESTO-

DISCUSION DEL ALGORITMO
El algoritmo ha sido diseñado a partir de resultados coincidentes en estudios y guías de práctica clínica.
En el contexto del sobreuso de TC cerebral en urgencias ante síncope, con muy baja rentabilidad diagnóstica, se observa la necesidad de adecuar la solicitud de TC siendo de indicación ante la sospecha diagnóstica de ACV / HSA.
En la revisión de la literatura se encuentra amplia información sobre la definición de síncope, su abordaje inicial en urgencias y posterior estudio en las sospechas de etiología cardiaca. En estos documentos y guías de sociedades de cardiología de diferentes procedencias, se facilita una definición común del evento, así como unanimidad en cuanto al bajo porcentaje de síncope de etiología neurológica en torno al 1% en todas las publicaciones y añadiendo que es siempre acompañado, o precedido de síntomas de focalidad y/o cefalea en todas las situaciones que precisa valoración neurológica y TC craneal, para descartar ACV en presentación de AIT o hemorragia subaracnoidea.
El algoritmo a pesar de no sostenerse sobre reglas de predicción clínica ya establecidas, sí se basa en datos y evidencia científica de diferente nivel coincidente en todos los textos revisados sin ninguna recomendación discordante.
Sobre estas premisas se diseña el algoritmo expuesto que indica solicitar TC craneal en aquellos episodios de síncope atendidos en urgencias únicamente en el caso de que estén acompañados de alguno de los considerados factores de alarma como la focalidad neurológica.
REFERENCIAS BIBLIOGRÁFICAS
Summaries
Up To Date:
- Author:David Benditt, Section Editors:Peter Kowey, Robert S Hockberger, Deputy Editor:Brian C Downey, Evaluation of syncope in adults. Clinical manifestations and diagnostic evaluation. Literature review current through: Jun 2018.
- Authors:Daniel McDermott, MD, James Quinn, MD, MS Section Editor:Robert S Hockberger, MD, FACEP Deputy Editor:Jonathan Grayzel, MD, FAAEM. Approach to the adult patient with syncope in the emergency department. Literature review current through: Jun 2018
Guidelines:
-Moya A, Sutton R, Ammirati F, Blanc JJ, Brignole M, Dahm JB, et al. European Society of Cardiology (ESC) guideline on diagnosis and management of syncope 2009. Eur Heart J. 2009; 30(21):2631-71.
-Strickberger SA, Benson DW, Biaggioni I, Callans DJ, Cohen MI, Ellenbogen KA, et al. American Heart Association/American College of Cardiology Foundation (AHA/ACCF) scientific statement on evaluation of syncope. Circulation 2006; 113(2):316.
–Giles MF, Albers GW, Amarenco P, Arsava EM, Asimos AW, Ay H, et al. Early stroke risk and ABCD2 score performance in tissue- vs time-defined TIA: a multicenter study. Neurology.2011; 77(13):1222-8.
–Arsava EM, Furie KL, Schwamm LH, Sorensen AG, Ay H. Prediction of early stroke risk in transient symptoms with infarction: relevance to the new tissue-based definition. Stroke.201; 42(8):2186-90.
-Alboni P, Brignole M, Menozzi C, Raviele A, Del Rosso A, Dinelli M, et al. Diagnostic value of history in patients with syncope with or without heart disease. Coll Cardiolog. 2001; 37(7):1921-8.
-Westby M, Davis S, Bullock I, Miller P, Cooper P , Turnbull N, Beal R, Braine M, Fear J, Goodwin M, Grünewald R, Jelen P Pawelec J, Petkar S, Pitcher D, Pottle A, Rogers G, Swann G (2010) Transient loss of consciousness (‘blackouts’) management in adults and young people. London: National Clinical Guideline Centre for Acute and Chronic Conditions, Royal College of Physicians.
– ACEP Clinical Policies Committee; Clinical Policies Subcommittee on Seizures. Clinical Policy: Critical issues in evaluation and management of adult patients presenting to emergency department with syncope. Ann Emerg Med 2007; 49(4):431.
Otras referencias Bibliográficas
- Thiruganasambandamoorthy V., Wells G.A., Hess E.P., Turko E., Perry J.J., Stiell I.G. Derivation of a risk scale and quantification of risk factors for serious adverse events in adult emergency department syncope patients. 2014 Mar;16(2):120-30,
- Stiell IG, Sivilotti MLA, Murray H, Rowe BH, Lang E, McRae A, et al. Risk stratification of adult emergency department syncope patients to predict short-term serious outcomes after discharge (RiSEDS) study. BMC emerg med. 2014; 14(100968543):8.
- Sim TB, Thng SY. Validation of the San Francisco Syncope Rule in two hospital emergency departments in an Asian population. Acad Emerg Med. 2013; 20(5):487–97.
- Quinn J.V., Stiell I.G., McDermott D.A., Sellers K.L., Kohn M.A., Wells G.A. Derivation of the San Francisco Syncope Rule to Predict Patients with Short-Term Serious Outcomes. Ann Emerg Med. 2004; 43(2):224-32.
- Kelly A-M, Kerr D. External validation of the San Francisco Syncope Rule in the Australian context. CJEM, Can j emerg med care. 2007; 9(3):157–61.
- Esses D, Bijur P, Wollowitz A, Gallagher EJ. Failure to validate the San Francisco Syncope Rule in an independent emergency department population. Ann Emerg Med. 2008; 52(2):151–9.
- Grossman S.A., Fischer C., Lipsitz L.A., Mottley L., Sands K., Thompson S., et al. Predicting Adverse Outcomes in Syncope. J Emerg Med. 2007; 33(3):233-9.
- Bar J, Fischer C, Lipsitz LA, Mottley L, Sands K, Zimetbaum P, et al. Reducing admissions utilizing the Boston Syncope Criteria. J Emerg Med. 2012; 42(3):345–52.
- Peeters SYG, Hoek AE, Mollink SM, Huff JS. Syncope: risk stratification and clinical decision making. Emerg med pract. 2014; 16(4):1–3.
- Davis J, Sen B, Shipsey D, Louw SJ, Dyker AG, Davis M, et al. The Recognition of Stroke in the Emergency Room (ROSIER) scale: development and validation of a stroke recognition instrument. Lancet neurol. 2005; 4(11):727–34.
- Whittaker R. The San Francisco Syncope Rule performs well in a regional rural emergency department in New Zealand. N Z Med J. 2013; 126(1374):29–33.
- Fischer C, Bar JL, Lipsitz LA, Mottley L, Sands K, Thompson S, et al. The yield of head CT in syncope: a pilot study. Intern emerg medicine. 2007; 2(1):46–9.
- Tan C., Sim T.B., Thng S.Y. Validation of the San Francisco syncope rule in two local hospitals emergency departments. Acad Emerg Med. 2013; 20(5):487-97.
ANEXO 1- ALGORITMO INFORMÁTICO